Daniel Gilbert Uchendu, Basil Nwaneri Okeahialam, Lucius Chidiebere Imoh, Abene Ezekiel Esala, Gimba Mark Zunman
{"title":"Type 2 Cardiorenal Syndrome: Prevalence and Correlates in Nigerian Heart Failure Patients.","authors":"Daniel Gilbert Uchendu, Basil Nwaneri Okeahialam, Lucius Chidiebere Imoh, Abene Ezekiel Esala, Gimba Mark Zunman","doi":"10.71480/nmj.v66i2.731","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Type 2 cardiorenal syndrome (Type 2 CRS) describes a relationship in which chronic congestive heart failure causes a progressive and permanent chronic kidney disease. Heart failure (HF) and chronic kidney disease (CKD) share similar cardiovascular risk factors and have a bi-directional relationship. A comprehensive approach including early screening of HF patients for CKD as well as management involving the nephrologist and cardiologist will most definitely reduce morbidity and mortality. The aim of this study was to determine the prevalence of and correlates for Type 2 CRS among HF patients in JUTH, Jos-Nigeria.</p><p><strong>Methodology: </strong>A hospital-based cross-sectional descriptive study carried out in JUTH involving 120 patients with chronic HF recruited consecutively. History, physical examination and laboratory investigations including urinalysis using albustix were performed on all subjects. CKD was determined using estimated glomerular function rate (eGFR) and persistent albuminuria. The data were analyzed using Epi Info (CDC, Atlanta GA) and p-values <0.05 were considered statistically significant.</p><p><strong>Results: </strong>The mean age of the participants was 52.00 ± 11.44 years, majority of whom were females consisting of 58.3%. The prevalence of CRS was 37.5%. Majoity (66.7%) of the patients had mild CRS, while 26.7% had moderate CRS, and only 6.7% had the severe CRS. The predictors of CRS were diabetes (OR=6.230; CI=2.094-19.093), New York heart Association (NYHA) grading I (OR=0.017; CI=0.002-0.142) and II (OR=0.089; CI=0.016-0.483), raised jugular venous pressure (JVP) (OR=7.099; CI=2.671-18.865), loud pulmonary component of the second heart sound (P2) (OR=3.769; CI=1.726-8.232), systolic dysfunction (EF<45%) (OR=3.316; CI=1.487-7.395), anaemia (OR=5.091; CI=1.657-15.640), albuminuria (OR:0.014, CI=0.004-0.052), rural/suburban dwelling (OR=2.875; CI=1.335-6.192) and increased cardiothoracic ratio (CTR) (OR=3.237; CI=1.019-10.278).</p><p><strong>Conclusion: </strong>The frequency of Type 2 CRS among CHF patients in JUTH was high. The predictors of chronic CRS include diabetes mellitus, NYHA grade, raised JVP, loud P2, systolic dysfunction, anaemia, albuminuria, rural/suburban dwelling and increased CTR. These findings highlight the urgent need to incorporate screening for CKD among stable heart failure patients at regular intervals, and early referral to the nephrologist to prevent further deterioration to ESRD.</p>","PeriodicalId":94346,"journal":{"name":"Nigerian medical journal : journal of the Nigeria Medical Association","volume":"66 2","pages":"607-620"},"PeriodicalIF":0.0000,"publicationDate":"2025-06-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12280315/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Nigerian medical journal : journal of the Nigeria Medical Association","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.71480/nmj.v66i2.731","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Type 2 cardiorenal syndrome (Type 2 CRS) describes a relationship in which chronic congestive heart failure causes a progressive and permanent chronic kidney disease. Heart failure (HF) and chronic kidney disease (CKD) share similar cardiovascular risk factors and have a bi-directional relationship. A comprehensive approach including early screening of HF patients for CKD as well as management involving the nephrologist and cardiologist will most definitely reduce morbidity and mortality. The aim of this study was to determine the prevalence of and correlates for Type 2 CRS among HF patients in JUTH, Jos-Nigeria.
Methodology: A hospital-based cross-sectional descriptive study carried out in JUTH involving 120 patients with chronic HF recruited consecutively. History, physical examination and laboratory investigations including urinalysis using albustix were performed on all subjects. CKD was determined using estimated glomerular function rate (eGFR) and persistent albuminuria. The data were analyzed using Epi Info (CDC, Atlanta GA) and p-values <0.05 were considered statistically significant.
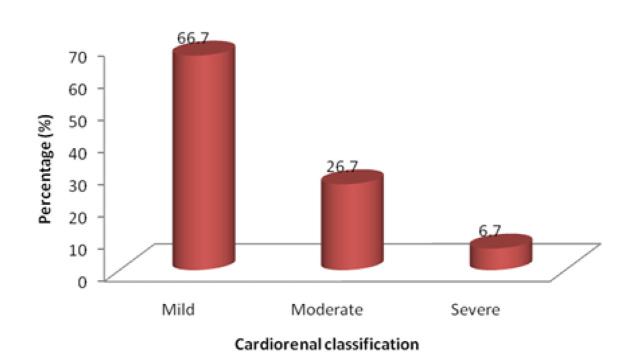
Results: The mean age of the participants was 52.00 ± 11.44 years, majority of whom were females consisting of 58.3%. The prevalence of CRS was 37.5%. Majoity (66.7%) of the patients had mild CRS, while 26.7% had moderate CRS, and only 6.7% had the severe CRS. The predictors of CRS were diabetes (OR=6.230; CI=2.094-19.093), New York heart Association (NYHA) grading I (OR=0.017; CI=0.002-0.142) and II (OR=0.089; CI=0.016-0.483), raised jugular venous pressure (JVP) (OR=7.099; CI=2.671-18.865), loud pulmonary component of the second heart sound (P2) (OR=3.769; CI=1.726-8.232), systolic dysfunction (EF<45%) (OR=3.316; CI=1.487-7.395), anaemia (OR=5.091; CI=1.657-15.640), albuminuria (OR:0.014, CI=0.004-0.052), rural/suburban dwelling (OR=2.875; CI=1.335-6.192) and increased cardiothoracic ratio (CTR) (OR=3.237; CI=1.019-10.278).
Conclusion: The frequency of Type 2 CRS among CHF patients in JUTH was high. The predictors of chronic CRS include diabetes mellitus, NYHA grade, raised JVP, loud P2, systolic dysfunction, anaemia, albuminuria, rural/suburban dwelling and increased CTR. These findings highlight the urgent need to incorporate screening for CKD among stable heart failure patients at regular intervals, and early referral to the nephrologist to prevent further deterioration to ESRD.
背景:2型心肾综合征(Type 2 CRS)描述了慢性充血性心力衰竭导致进行性和永久性慢性肾脏疾病的关系。心衰(HF)和慢性肾脏疾病(CKD)具有相似的心血管危险因素,并具有双向关系。包括心衰患者CKD早期筛查以及肾病专家和心脏病专家参与的管理在内的综合方法肯定会降低发病率和死亡率。本研究的目的是确定乔斯-尼日利亚JUTH地区HF患者中2型CRS的患病率及其相关因素。方法:在JUTH开展了一项基于医院的横断面描述性研究,连续招募了120例慢性心衰患者。对所有受试者进行病史、体格检查和实验室调查,包括使用albustix进行尿液分析。通过肾小球功能率(eGFR)和持续蛋白尿来确定CKD。数据采用Epi Info (CDC, Atlanta GA)和p值分析结果:参与者平均年龄为52.00±11.44岁,以女性为主,占58.3%;CRS患病率为37.5%。轻度CRS占多数(66.7%),中度CRS占26.7%,重度CRS仅占6.7%。CRS的预测因子为糖尿病(OR=6.230;CI=2.094-19.093),纽约心脏协会(NYHA)分级I级(OR=0.017;CI=0.002-0.142)和II (OR=0.089;CI=0.016-0.483),颈静脉压升高(JVP) (OR=7.099;CI=2.671-18.865),第二心音肺分量大(P2) (OR=3.769;CI=1.726-8.232)、收缩功能障碍(eff)。结论:JUTH期CHF患者发生2型CRS的频率较高。慢性CRS的预测因素包括糖尿病、NYHA分级、JVP升高、P2升高、收缩功能障碍、贫血、蛋白尿、农村/郊区居住和CTR升高。这些发现强调了在稳定型心衰患者中定期筛查CKD的迫切需要,以及早期转诊到肾病科以防止进一步恶化为ESRD。


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


