Kyriaki Astara, Maria Lypiridou, Konstantinos Kalafatakis, Georgios Nikolaou, Georgios Stouraitis
{"title":"Neuromyelitis Optica Diagnosis in Two Elderly Patients with Systematic Lupus Erythematosus: A Case Series.","authors":"Kyriaki Astara, Maria Lypiridou, Konstantinos Kalafatakis, Georgios Nikolaou, Georgios Stouraitis","doi":"10.3390/reports8030110","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background and Clinical Significance:</b> Neuromyelitis optica (NMO) is a chronic demyelinating inflammatory disease of the central nervous system (CNS), mediated by autoantibodies against aquaporin-4 (AQ4) receptors. In the spectrum of NMO, other autoimmune diseases also coexist, though their association with systemic lupus erythematosus (SLE) is rare. <b>Case Presentation:</b> We present two cases of patients in their 70s who were diagnosed with NMO in the context of SLE. The first case concerns a 78-year-old woman with drug-induced SLE and thoracic myelitis who developed T4-level incomplete paraplegia over three weeks. The second case involves a 71-year-old woman with a history of SLE and myasthenia gravis, presenting with cervical myelitis with progressive worsening of walking and C4-level paraparesis over two months. In both cases, elevated serum anti-AQ4 titers were detected, establishing the diagnosis of NMO and differentiation from an atypical manifestation of SLE-related myelitis. High doses of intravenous corticosteroids with gradual tapering, along with cyclophosphamide, followed by rituximab, were administered in both patients. The first patient showed a poor response, while the second showed improvement. <b>Conclusions:</b> The coexistence of NMO with SLE is rare, but the occurrence of myelitis in patients with connective tissue diseases should raise the suspicion of NMO, especially in elderly women and several years after the diagnosis of SLE. Time to treatment is critical, as delays in treating NMO can result in cumulative and disabling damage.</p>","PeriodicalId":74664,"journal":{"name":"Reports (MDPI)","volume":"8 3","pages":""},"PeriodicalIF":0.8000,"publicationDate":"2025-07-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12265998/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Reports (MDPI)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/reports8030110","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
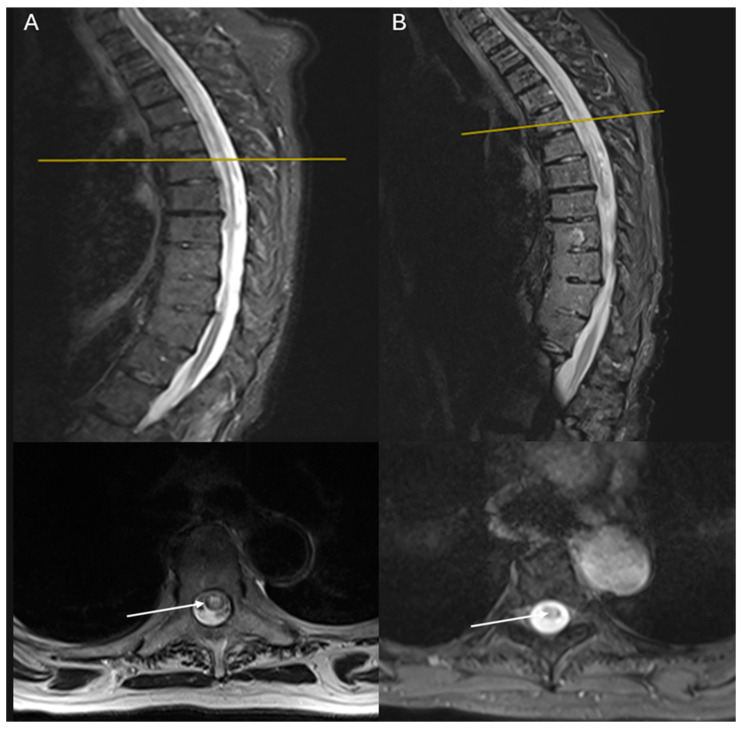
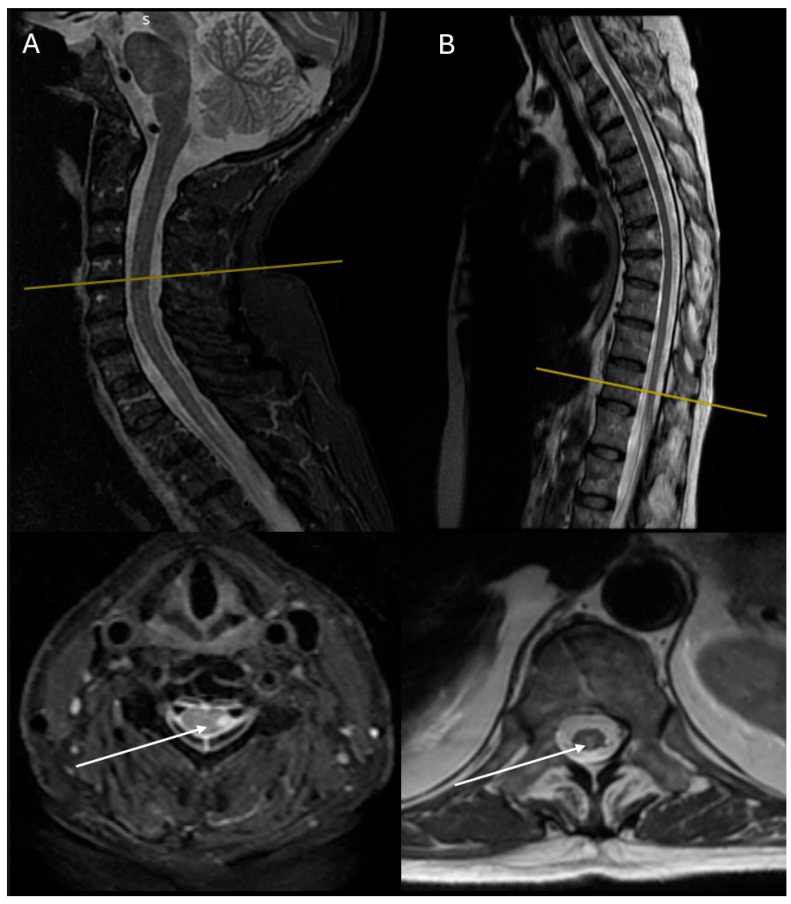
Background and Clinical Significance: Neuromyelitis optica (NMO) is a chronic demyelinating inflammatory disease of the central nervous system (CNS), mediated by autoantibodies against aquaporin-4 (AQ4) receptors. In the spectrum of NMO, other autoimmune diseases also coexist, though their association with systemic lupus erythematosus (SLE) is rare. Case Presentation: We present two cases of patients in their 70s who were diagnosed with NMO in the context of SLE. The first case concerns a 78-year-old woman with drug-induced SLE and thoracic myelitis who developed T4-level incomplete paraplegia over three weeks. The second case involves a 71-year-old woman with a history of SLE and myasthenia gravis, presenting with cervical myelitis with progressive worsening of walking and C4-level paraparesis over two months. In both cases, elevated serum anti-AQ4 titers were detected, establishing the diagnosis of NMO and differentiation from an atypical manifestation of SLE-related myelitis. High doses of intravenous corticosteroids with gradual tapering, along with cyclophosphamide, followed by rituximab, were administered in both patients. The first patient showed a poor response, while the second showed improvement. Conclusions: The coexistence of NMO with SLE is rare, but the occurrence of myelitis in patients with connective tissue diseases should raise the suspicion of NMO, especially in elderly women and several years after the diagnosis of SLE. Time to treatment is critical, as delays in treating NMO can result in cumulative and disabling damage.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


