Marcin Sota, Daria Bramnik, Olivia Gudziewski, Ithamar Cheyne, Małgorzata Mikaszewska-Sokolewicz
{"title":"High-Stakes Hormone: Vasopressin Use as a Last-Line Therapy for Shock in Pediatrics-A Narrative Review.","authors":"Marcin Sota, Daria Bramnik, Olivia Gudziewski, Ithamar Cheyne, Małgorzata Mikaszewska-Sokolewicz","doi":"10.3390/reports8030117","DOIUrl":null,"url":null,"abstract":"<p><p>Background and Clinical Significance: Shock in pediatric patients remains a leading cause of morbidity and mortality, with refractory cases posing significant challenges. While catecholamines like norepinephrine and epinephrine are standard vasopressors, vasopressin (AVP) has emerged as a potential adjunct therapy. However, its role in pediatric shock remains controversial due to concerns about efficacy, safety, and appropriate use. This review assesses the current evidence on AVP in pediatric shock. Methods and Results: A comprehensive literature search was conducted using PubMed, Scopus, Web of Science, and Google Scholar, focusing on studies published in the last five years to capture recent advancements. Articles on AVP's mechanism of action, pharmacokinetics, clinical applications, and safety were included. For background information, studies were not limited by publication date. AVP increases mean arterial pressure (MAP) and systemic vascular resistance (SVR) yet does not significantly reduce mortality. While AVP may be useful in catecholamine-resistant vasoplegia, its advantage over conventional vasopressors remains uncertain. Concerns about ischemic complications, myocardial dysfunction, and thrombocytopenia further limit its routine use. Conclusions: AVP may serve as an adjunct therapy in catecholamine-resistant vasoplegia, but safety concerns and unclear benefits restrict its routine use. Further research is needed to determine the optimal dosing, patient selection, and long-term outcomes. Until then, AVP should remain a last-line therapy when conventional vasopressors fail.</p>","PeriodicalId":74664,"journal":{"name":"Reports (MDPI)","volume":"8 3","pages":""},"PeriodicalIF":0.8000,"publicationDate":"2025-07-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12286069/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Reports (MDPI)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/reports8030117","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
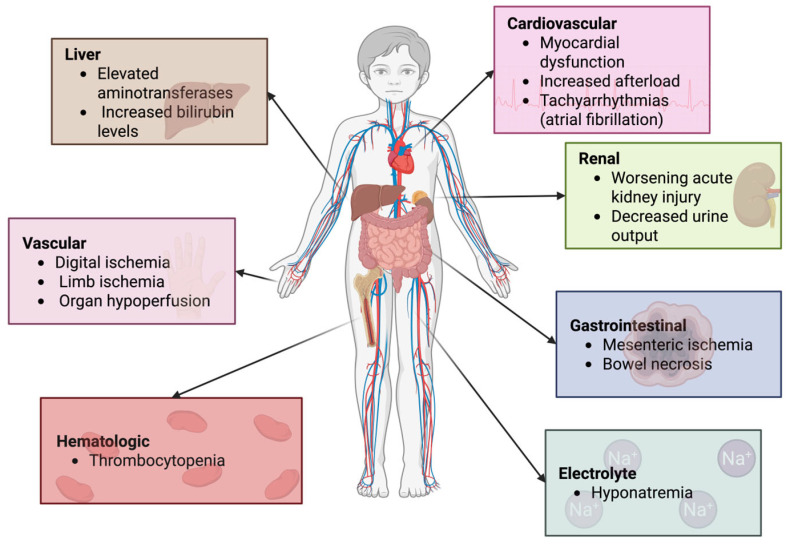
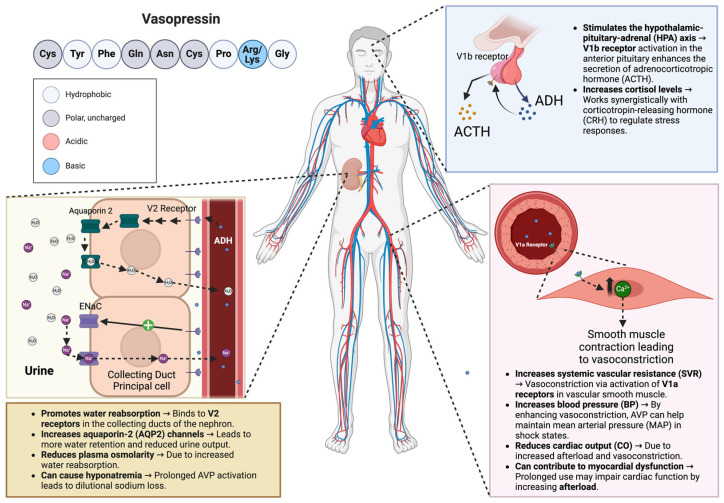
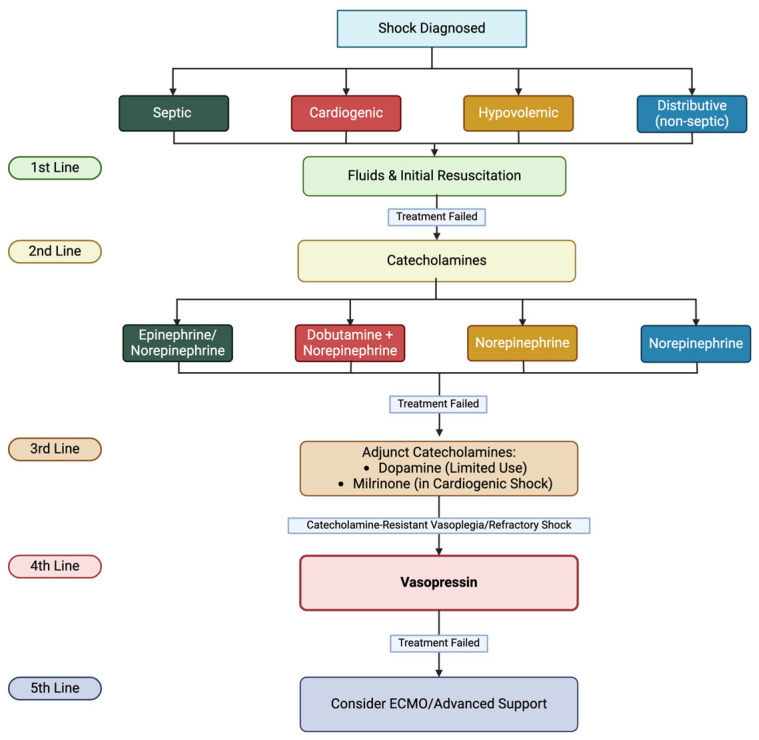
Background and Clinical Significance: Shock in pediatric patients remains a leading cause of morbidity and mortality, with refractory cases posing significant challenges. While catecholamines like norepinephrine and epinephrine are standard vasopressors, vasopressin (AVP) has emerged as a potential adjunct therapy. However, its role in pediatric shock remains controversial due to concerns about efficacy, safety, and appropriate use. This review assesses the current evidence on AVP in pediatric shock. Methods and Results: A comprehensive literature search was conducted using PubMed, Scopus, Web of Science, and Google Scholar, focusing on studies published in the last five years to capture recent advancements. Articles on AVP's mechanism of action, pharmacokinetics, clinical applications, and safety were included. For background information, studies were not limited by publication date. AVP increases mean arterial pressure (MAP) and systemic vascular resistance (SVR) yet does not significantly reduce mortality. While AVP may be useful in catecholamine-resistant vasoplegia, its advantage over conventional vasopressors remains uncertain. Concerns about ischemic complications, myocardial dysfunction, and thrombocytopenia further limit its routine use. Conclusions: AVP may serve as an adjunct therapy in catecholamine-resistant vasoplegia, but safety concerns and unclear benefits restrict its routine use. Further research is needed to determine the optimal dosing, patient selection, and long-term outcomes. Until then, AVP should remain a last-line therapy when conventional vasopressors fail.
背景和临床意义:儿科患者休克仍然是发病率和死亡率的主要原因,难治性病例提出了重大挑战。儿茶酚胺如去甲肾上腺素和肾上腺素是标准的抗利尿激素,抗利尿激素(AVP)已成为一种潜在的辅助治疗药物。然而,由于对其有效性、安全性和适当使用的担忧,其在小儿休克中的作用仍然存在争议。本综述评估了目前关于小儿休克中AVP的证据。方法与结果:使用PubMed、Scopus、Web of Science和b谷歌Scholar进行了全面的文献检索,重点关注最近五年发表的研究,以获取最新进展。文章包括AVP的作用机制、药代动力学、临床应用和安全性。关于背景资料,研究不受出版日期的限制。AVP增加平均动脉压(MAP)和全身血管阻力(SVR),但没有显著降低死亡率。虽然AVP可能对儿茶酚胺抗性血管截瘫有用,但其优于传统血管加压药物的优势仍不确定。对缺血性并发症、心肌功能障碍和血小板减少症的担忧进一步限制了其常规应用。结论:AVP可作为儿茶酚胺抵抗性血管截瘫的辅助治疗,但安全性问题和不明确的疗效限制了其常规应用。需要进一步的研究来确定最佳剂量、患者选择和长期结果。在此之前,当传统的血管加压药物失效时,AVP仍然是最后的治疗方法。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


