Cardiac autonomic function score: a novel risk stratification tool in the cardiac intensive care unit based on periodic repolarization dynamics and deceleration capacity of heart rate (LMU-eICU study).
Mathias Klemm, Lukas von Stülpnagel, Valentin Ostermaier, Carsten Theurer, Laura E Villegas Sierra, Felix Wenner, Elodie Eiffener, Aresa Krasniqi, Konstantinos Mourouzis, Lauren E Sams, Luisa Freyer, Steffen Massberg, Axel Bauer, Konstantinos D Rizas
{"title":"Cardiac autonomic function score: a novel risk stratification tool in the cardiac intensive care unit based on periodic repolarization dynamics and deceleration capacity of heart rate (LMU-eICU study).","authors":"Mathias Klemm, Lukas von Stülpnagel, Valentin Ostermaier, Carsten Theurer, Laura E Villegas Sierra, Felix Wenner, Elodie Eiffener, Aresa Krasniqi, Konstantinos Mourouzis, Lauren E Sams, Luisa Freyer, Steffen Massberg, Axel Bauer, Konstantinos D Rizas","doi":"10.1093/ehjdh/ztaf038","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Treatment capacities on intensive care units (ICUs) are a limited resource reserved for high-risk patients. To facilitate risk stratification of ICU patients, several scoring systems have been developed over time. Among them, the Simplified Acute Physiology Score 3 (SAPS3) is the gold standard, but lacks specificity for cardiac ICU patients. Here, we propose a novel, fully automated, electrocardiogram-based cardiac autonomic risk stratification score (CAF<sub>ICU</sub>) that substantially adds to current risk stratification strategies.</p><p><strong>Methods and results: </strong>CAF<sub>ICU</sub> is based on periodic repolarization dynamics, a marker of sympathetic overactivity and deceleration capacity of heart rate, a parameter of vagal imbalance. We developed CAF<sub>ICU</sub> in a retrospective cohort of 355 ICU patients and subsequently validated the score in a cohort of 702 ICU patients, enrolled between February-November 2018 and December 2018-April 2020 at a large cardiac ICU in a tertiary hospital. The primary endpoint of the study was 30-day intrahospital mortality. Thirty (8.5%) and 100 (14.2%) patients reached the primary endpoint in the training and validation cohorts, respectively. CAF<sub>ICU</sub> was significantly higher in non-survivors than survivors (2.58 ± 1.34 vs. 1.76 ± 0.97 units; <i>P</i> = 0.003 in the training cohort and 2.20 ± 1.05 vs. 1.70 ± 0.83 units; <i>P</i> < 0.001 in the validation cohort) and was a strong predictor of mortality in both the training [hazard ratio (HR) 25.67; 95% confidence interval (CI) 3.50-188.40; <i>P</i> = 0.001] and validation cohorts (HR 4.70; 95% CI 2.79-7.92; <i>P</i> < 0.001). In the pooled cohort, CAF<sub>ICU</sub> significantly improved risk stratification based on SAPS3 (IDI-increase 0.033; 95% CI 0.010-0.061; <i>P</i> < 0.001).</p><p><strong>Conclusion: </strong>ECG-based automatic autonomic risk stratification by means of PRD and DC is highly predictive of short-term mortality in the ICU and can be combined with the SAPS3-Score to identify patients with increased risk for intrahospital mortality. This method can be integrated in conventional monitors and may improve risk stratification strategies in cardiac ICUs.</p>","PeriodicalId":72965,"journal":{"name":"European heart journal. Digital health","volume":"6 4","pages":"822-832"},"PeriodicalIF":4.4000,"publicationDate":"2025-04-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12282351/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal. Digital health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjdh/ztaf038","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
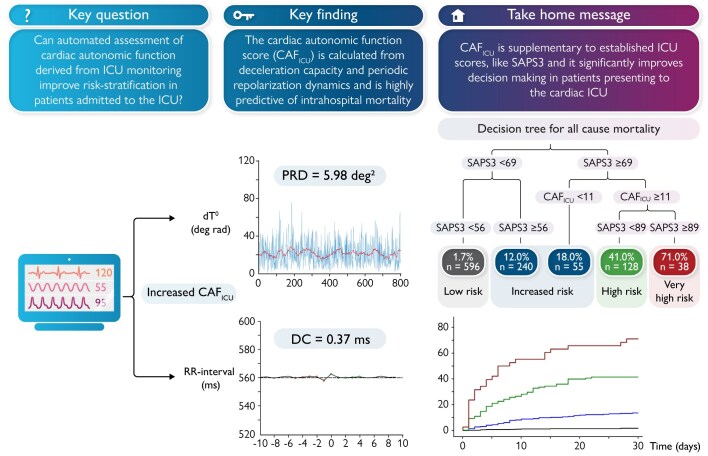
Aims: Treatment capacities on intensive care units (ICUs) are a limited resource reserved for high-risk patients. To facilitate risk stratification of ICU patients, several scoring systems have been developed over time. Among them, the Simplified Acute Physiology Score 3 (SAPS3) is the gold standard, but lacks specificity for cardiac ICU patients. Here, we propose a novel, fully automated, electrocardiogram-based cardiac autonomic risk stratification score (CAFICU) that substantially adds to current risk stratification strategies.
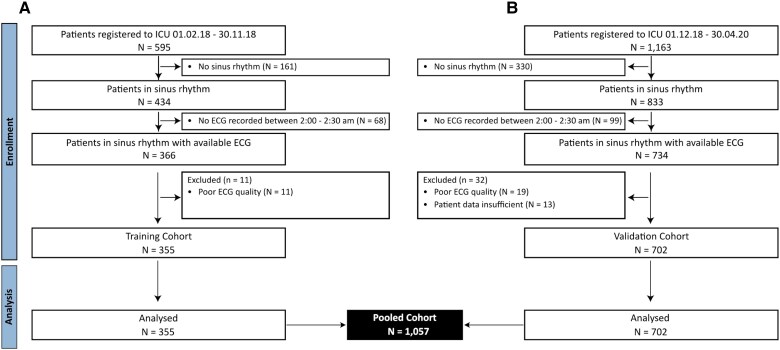
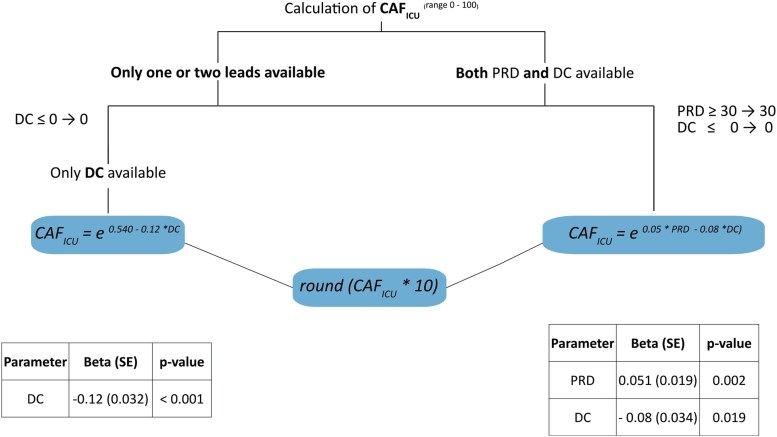
Methods and results: CAFICU is based on periodic repolarization dynamics, a marker of sympathetic overactivity and deceleration capacity of heart rate, a parameter of vagal imbalance. We developed CAFICU in a retrospective cohort of 355 ICU patients and subsequently validated the score in a cohort of 702 ICU patients, enrolled between February-November 2018 and December 2018-April 2020 at a large cardiac ICU in a tertiary hospital. The primary endpoint of the study was 30-day intrahospital mortality. Thirty (8.5%) and 100 (14.2%) patients reached the primary endpoint in the training and validation cohorts, respectively. CAFICU was significantly higher in non-survivors than survivors (2.58 ± 1.34 vs. 1.76 ± 0.97 units; P = 0.003 in the training cohort and 2.20 ± 1.05 vs. 1.70 ± 0.83 units; P < 0.001 in the validation cohort) and was a strong predictor of mortality in both the training [hazard ratio (HR) 25.67; 95% confidence interval (CI) 3.50-188.40; P = 0.001] and validation cohorts (HR 4.70; 95% CI 2.79-7.92; P < 0.001). In the pooled cohort, CAFICU significantly improved risk stratification based on SAPS3 (IDI-increase 0.033; 95% CI 0.010-0.061; P < 0.001).
Conclusion: ECG-based automatic autonomic risk stratification by means of PRD and DC is highly predictive of short-term mortality in the ICU and can be combined with the SAPS3-Score to identify patients with increased risk for intrahospital mortality. This method can be integrated in conventional monitors and may improve risk stratification strategies in cardiac ICUs.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


