Abdullah Alrumayh, Patrik Bächtiger, Arunashis Sau, Josephine Mansell, Melanie T Almonte, Karanjot Chhatwal, Fu Siong Ng, Mihir A Kelshiker, Nicholas S Peters
{"title":"Artificial intelligence analysis of the single-lead ECG predicts long-term clinical outcomes.","authors":"Abdullah Alrumayh, Patrik Bächtiger, Arunashis Sau, Josephine Mansell, Melanie T Almonte, Karanjot Chhatwal, Fu Siong Ng, Mihir A Kelshiker, Nicholas S Peters","doi":"10.1093/ehjdh/ztaf057","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Artificial intelligence (AI) applied to a single-lead electrocardiogram (AI-ECG) can detect impaired left ventricular systolic dysfunction [LVSD: left ventricular ejection fraction (LVEF) ≤ 40%]. This study aimed to determine if AI-ECG can also predict the two-year risk of major adverse cardiovascular events (MACE) and all-cause mortality independent of LVSD.</p><p><strong>Methods and results: </strong>Clinical outcomes after two-year follow-up were collected on patients who attended for routine echocardiography and received simultaneous single-lead-ECG recording for AI-ECG analysis. MACE and all-cause mortality were compared by Cox regression, measured against the classification of LVEF > or ≤40%. A subgroup analysis was performed on patients with echocardiographic LVEF ≥ 50%. With previously established thresholds, 'positive' AI-ECG was defined as an LVEF-predicted ≤40%, and negative AI-ECG signified an LVEF-predicted >40%; 1007 patients were included for analysis (mean age, 62.3 years; 52.4% male). 339 (33.7%) had an AI-ECG-predicted LVEF ≤ 40% and had a higher MACE rate (LVEF ≤ 40% vs. >40%: 34.2% vs.11.9%; adjusted hazard ratio (aHR) 1.93; 95% CI, 1.39-2.69; <i>P</i> < 0.001), primarily driven by increased mortality (23% vs. 9.6%; <i>P</i> < 0.001; aHR 1.56; 95% CI, 1.06-2.29; <i>P</i> = 0.0239). In patients with echocardiographic LVEF ≥ 50%, there was a higher incidence of MACE in those with an AI-ECG 'false positive' prediction of LVEF ≤ 40% (27.2% vs.11.9%; <i>P</i> < 0.001; aHR 1.71 and 95% CI, 1.11-2.47) and all-cause mortality (20.4% vs. 9.6%; <i>P</i> < 0.001; aHR 1.59, 95% CI, 1.09-2.42).</p><p><strong>Conclusion: </strong>An AI-ECG algorithm designed to detect LVEF ≤ 40% can also identify patients at risk of MACE and all-cause mortality from single-lead ECG recording-independent of actual LVEF on echo. This requires further evaluation as a point-of-care risk stratification tool.</p>","PeriodicalId":72965,"journal":{"name":"European heart journal. Digital health","volume":"6 4","pages":"635-644"},"PeriodicalIF":4.4000,"publicationDate":"2025-06-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12282343/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal. Digital health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjdh/ztaf057","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
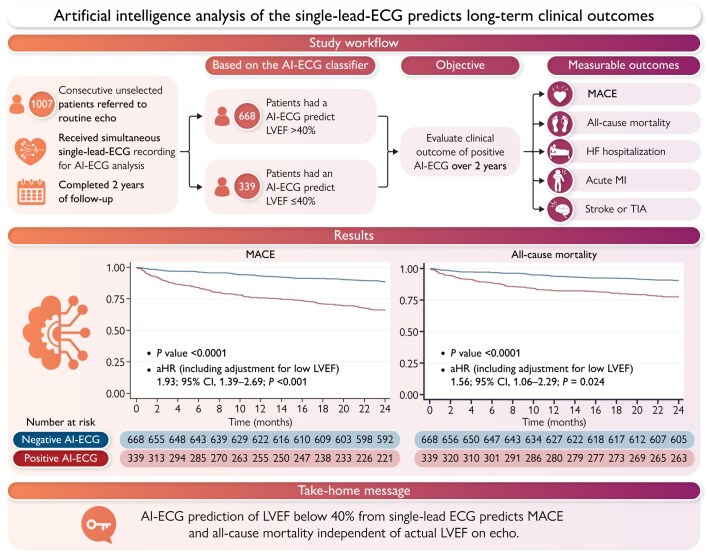
Aims: Artificial intelligence (AI) applied to a single-lead electrocardiogram (AI-ECG) can detect impaired left ventricular systolic dysfunction [LVSD: left ventricular ejection fraction (LVEF) ≤ 40%]. This study aimed to determine if AI-ECG can also predict the two-year risk of major adverse cardiovascular events (MACE) and all-cause mortality independent of LVSD.
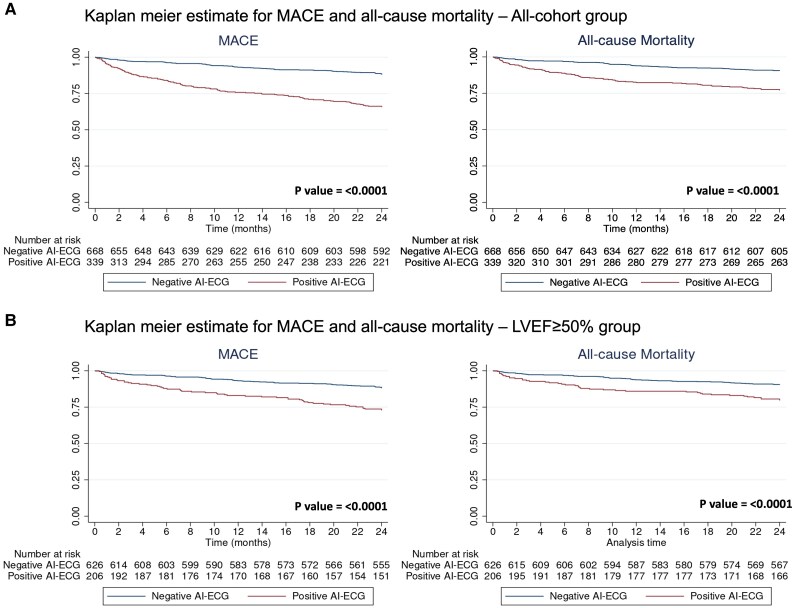
Methods and results: Clinical outcomes after two-year follow-up were collected on patients who attended for routine echocardiography and received simultaneous single-lead-ECG recording for AI-ECG analysis. MACE and all-cause mortality were compared by Cox regression, measured against the classification of LVEF > or ≤40%. A subgroup analysis was performed on patients with echocardiographic LVEF ≥ 50%. With previously established thresholds, 'positive' AI-ECG was defined as an LVEF-predicted ≤40%, and negative AI-ECG signified an LVEF-predicted >40%; 1007 patients were included for analysis (mean age, 62.3 years; 52.4% male). 339 (33.7%) had an AI-ECG-predicted LVEF ≤ 40% and had a higher MACE rate (LVEF ≤ 40% vs. >40%: 34.2% vs.11.9%; adjusted hazard ratio (aHR) 1.93; 95% CI, 1.39-2.69; P < 0.001), primarily driven by increased mortality (23% vs. 9.6%; P < 0.001; aHR 1.56; 95% CI, 1.06-2.29; P = 0.0239). In patients with echocardiographic LVEF ≥ 50%, there was a higher incidence of MACE in those with an AI-ECG 'false positive' prediction of LVEF ≤ 40% (27.2% vs.11.9%; P < 0.001; aHR 1.71 and 95% CI, 1.11-2.47) and all-cause mortality (20.4% vs. 9.6%; P < 0.001; aHR 1.59, 95% CI, 1.09-2.42).
Conclusion: An AI-ECG algorithm designed to detect LVEF ≤ 40% can also identify patients at risk of MACE and all-cause mortality from single-lead ECG recording-independent of actual LVEF on echo. This requires further evaluation as a point-of-care risk stratification tool.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


