David O Arnar, Bartosz Dobies, Elias F Gudmundsson, Heida B Bragadottir, Gudbjorg Jona Gudlaugsdottir, Audur Ketilsdottir, Hallveig Broddadottir, Brynja Laxdal, Thordis Jona Hrafnkelsdottir, Inga J Ingimarsdottir, Bylgja Kaernested, Axel F Sigurdsson, Ari Isberg, Svala Sigurdardottir, Tryggvi Thorgeirsson, Saemundur J Oddsson
{"title":"Effect of a digital health intervention on outpatients with heart failure: a randomized, controlled trial.","authors":"David O Arnar, Bartosz Dobies, Elias F Gudmundsson, Heida B Bragadottir, Gudbjorg Jona Gudlaugsdottir, Audur Ketilsdottir, Hallveig Broddadottir, Brynja Laxdal, Thordis Jona Hrafnkelsdottir, Inga J Ingimarsdottir, Bylgja Kaernested, Axel F Sigurdsson, Ari Isberg, Svala Sigurdardottir, Tryggvi Thorgeirsson, Saemundur J Oddsson","doi":"10.1093/ehjdh/ztaf063","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Heart failure (HF) is associated with high mortality and reduced quality of life (QoL). Interventions encouraging a healthy lifestyle and self-care can reduce morbidity and HF-related hospitalizations. We conducted a randomized controlled trial (RCT) to assess the impact of a digital health programme on QoL and clinical outcomes of patients. The programme included remote patient monitoring (RPM), self-care, HF education, and empowered positive lifestyle changes.</p><p><strong>Methods and results: </strong>Patients (<i>n</i> = 175) received standard-of-care (SoC) at a HF outpatient clinic (control, <i>n</i> = 89) or SoC plus a digital health programme (intervention, <i>n</i> = 86) for 6 months, followed by a 6-month maintenance period. Compliance with RPM was 93% at 6 months. No significant between-group difference was found in the primary endpoint (health-related QoL), except in an exploratory subgroup of New York Heart Association class III patients, where the intervention group had a significantly smaller QoL decline (<i>P</i> = 0.023). For secondary endpoints, the intervention group had significantly greater improvements in self-care at 6 months (<i>P</i> < 0.001) and 12 months (<i>P</i> = 0.003), and in disease-specific knowledge at 12 months (<i>P</i> = 0.001). Several exploratory endpoints favoured the intervention, with significant improvements in triglycerides (<i>P</i> = 0.012), HbA1c (<i>P</i> = 0.014), and fasting glucose (<i>P</i> = 0.010). The TG/HDL cholesterol ratio and TG/glucose index improved significantly at both 6 and 12 months in between-group comparisons.</p><p><strong>Conclusion: </strong>Although the digital programme did not improve health-related QoL, it led to benefits in other important outcomes such as self-care, disease-specific knowledge, and several key metabolic parameters.</p>","PeriodicalId":72965,"journal":{"name":"European heart journal. Digital health","volume":"6 4","pages":"749-762"},"PeriodicalIF":4.4000,"publicationDate":"2025-06-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12282350/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal. Digital health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjdh/ztaf063","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
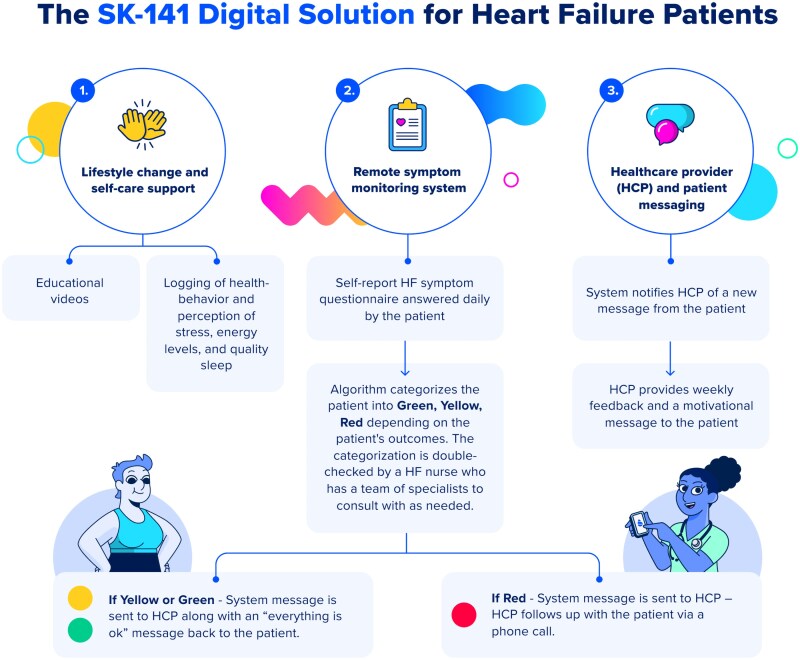
Aims: Heart failure (HF) is associated with high mortality and reduced quality of life (QoL). Interventions encouraging a healthy lifestyle and self-care can reduce morbidity and HF-related hospitalizations. We conducted a randomized controlled trial (RCT) to assess the impact of a digital health programme on QoL and clinical outcomes of patients. The programme included remote patient monitoring (RPM), self-care, HF education, and empowered positive lifestyle changes.
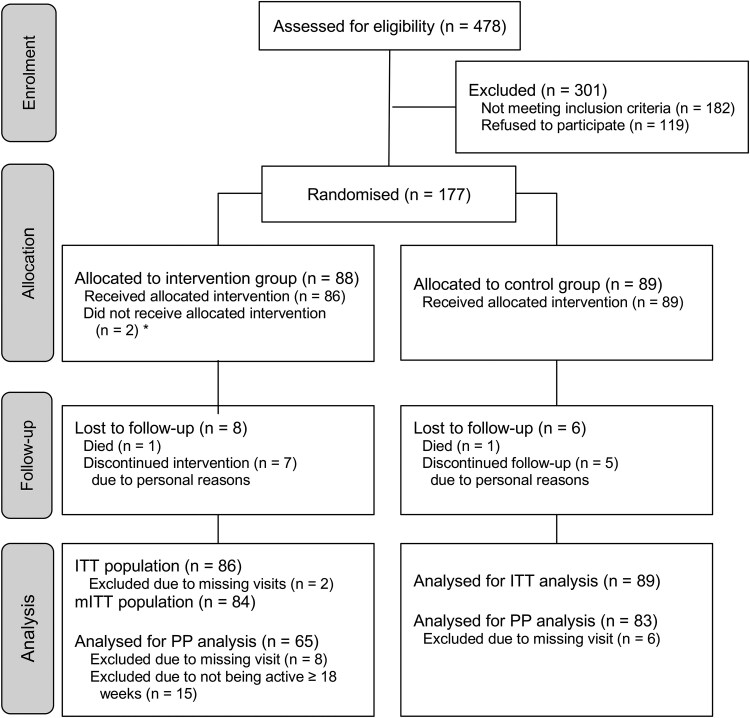
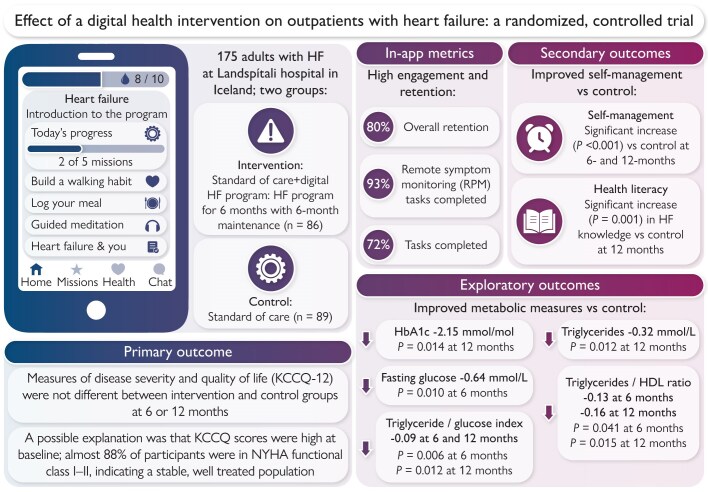
Methods and results: Patients (n = 175) received standard-of-care (SoC) at a HF outpatient clinic (control, n = 89) or SoC plus a digital health programme (intervention, n = 86) for 6 months, followed by a 6-month maintenance period. Compliance with RPM was 93% at 6 months. No significant between-group difference was found in the primary endpoint (health-related QoL), except in an exploratory subgroup of New York Heart Association class III patients, where the intervention group had a significantly smaller QoL decline (P = 0.023). For secondary endpoints, the intervention group had significantly greater improvements in self-care at 6 months (P < 0.001) and 12 months (P = 0.003), and in disease-specific knowledge at 12 months (P = 0.001). Several exploratory endpoints favoured the intervention, with significant improvements in triglycerides (P = 0.012), HbA1c (P = 0.014), and fasting glucose (P = 0.010). The TG/HDL cholesterol ratio and TG/glucose index improved significantly at both 6 and 12 months in between-group comparisons.
Conclusion: Although the digital programme did not improve health-related QoL, it led to benefits in other important outcomes such as self-care, disease-specific knowledge, and several key metabolic parameters.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


