Mohammed Halawani, Arwa Alsharif, Omar Ibrahim Alanazi, Baraa Awad, Abdulaziz Alsharif, Hawazen Alahmadi, Rayan Alqarni, Rahaf Mohammed Alhindi, Abdulmohsen H Alanazi, Abdulmajeed Hassan Alshamrani
{"title":"Efficacy and Safety of Adenotonsillectomy for Pediatric Obstructive Sleep Apnea Across Various Age Groups: A Systematic Review.","authors":"Mohammed Halawani, Arwa Alsharif, Omar Ibrahim Alanazi, Baraa Awad, Abdulaziz Alsharif, Hawazen Alahmadi, Rayan Alqarni, Rahaf Mohammed Alhindi, Abdulmohsen H Alanazi, Abdulmajeed Hassan Alshamrani","doi":"10.3390/pediatric17040071","DOIUrl":null,"url":null,"abstract":"<p><p><b>Objectives</b>: To assess the safety and efficacy of adenotonsillectomy (AT) for treating uncomplicated pediatric obstructive sleep apnea (OSA) in children of different ages. <b>Methods</b>: A systematic search was conducted in four electronic databases, and 71 studies with a total of 9087 participants were included in the analysis. The studies were all before-and-after studies, cohort studies, and randomized controlled trials. Surgical results were analyzed according to age, disease severity, and follow-up duration. <b>Results</b>: Children younger than 7 years at the time of AT had a significantly greater decrease in disease severity, a greater decrease in hypoxemic burden, improved sleep quality, and improved cardiovascular function than children older than 7 years. Both cognitive and behavioral performance improved postoperatively, although these changes were more significantly associated with the duration of follow-up than with age at surgery. Notably, the rate of surgical complications was much greater in children under the age of 3. <b>Conclusions</b>: The current evidence indicates that AT is performed optimally between the ages of 3 and 7 years, offering the greatest chance of disease resolution and remission of associated conditions, balanced with a reduction in surgical risk. We highly recommend conducting high-quality randomized controlled trials to further inform the clinical guidelines for pediatric AT.</p>","PeriodicalId":45251,"journal":{"name":"Pediatric Reports","volume":"17 4","pages":""},"PeriodicalIF":1.4000,"publicationDate":"2025-06-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12286109/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/pediatric17040071","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
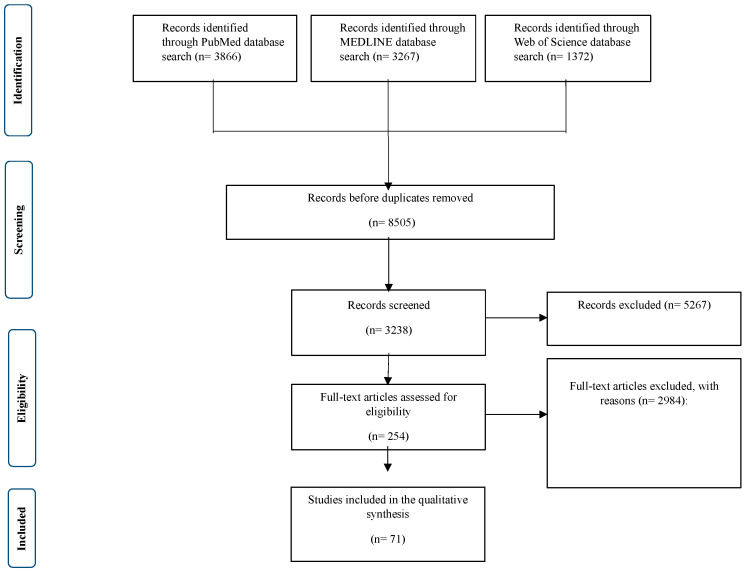
Objectives: To assess the safety and efficacy of adenotonsillectomy (AT) for treating uncomplicated pediatric obstructive sleep apnea (OSA) in children of different ages. Methods: A systematic search was conducted in four electronic databases, and 71 studies with a total of 9087 participants were included in the analysis. The studies were all before-and-after studies, cohort studies, and randomized controlled trials. Surgical results were analyzed according to age, disease severity, and follow-up duration. Results: Children younger than 7 years at the time of AT had a significantly greater decrease in disease severity, a greater decrease in hypoxemic burden, improved sleep quality, and improved cardiovascular function than children older than 7 years. Both cognitive and behavioral performance improved postoperatively, although these changes were more significantly associated with the duration of follow-up than with age at surgery. Notably, the rate of surgical complications was much greater in children under the age of 3. Conclusions: The current evidence indicates that AT is performed optimally between the ages of 3 and 7 years, offering the greatest chance of disease resolution and remission of associated conditions, balanced with a reduction in surgical risk. We highly recommend conducting high-quality randomized controlled trials to further inform the clinical guidelines for pediatric AT.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


