{"title":"Antibiotic Effect on Clinical Response and Remission in Pediatric Inflammatory Bowel Disease.","authors":"Caeley Dye, Caroline M Sierra, Khaled Bahjri, Mallory Cohen, Gautam Nagendra","doi":"10.3390/pediatric17040077","DOIUrl":null,"url":null,"abstract":"<p><p><b>Objective</b>: Gut dysbiosis has been implicated in the pathology of inflammatory bowel disease (IBD). There is some evidence to suggest that the use of antibiotic treatment can incite an early clinical response or remission when used in conjunction with standard-of-care (SOC) therapy to treat IBD-related flares. Furthermore, antibiotics have been historically investigated for use as a bridge when initiating biologic therapy while waiting for peak biologic treatment effect to occur. This study investigated and compared the time to clinical response when treated with combination antibiotics, metronidazole monotherapy, or SOC therapy in pediatric patients with an active IBD flare. <b>Methods</b>: This study was a retrospective, Institution Review Board-approved, single-centered cohort study which included patients who were less than 18 years of age with a confirmed diagnosis of IBD who received conventional treatment alone or with either combination antibiotic therapy or metronidazole monotherapy to treat an active IBD flare between March 2013 and January 2024. Patients were excluded if they received antibiotic therapy to treat an active infection, had positive stool cultures or enteric pathogen polymerase chain reaction panel, or had colonic disease limited to the rectum. <b>Results</b>: Fifty-nine patients were included and divided into metronidazole monotherapy (<i>n</i> = 18), SOC therapy (<i>n</i> = 20), and combination antibiotics (<i>n</i> = 21). The primary outcome of days to clinical response was not significantly different across all groups; however, patients who received combination antibiotics achieved the fastest time to clinical response (median (IRQ))-4 days (1, 65), compared to 7.5 days (1, 119) for the SOC group and 9 days (2, 217) for the metronidazole group. Secondary outcomes of achievement of clinical response, remission, or failure were determined to be non-significant between all groups. <b>Conclusions</b>: There is no significant difference in time to clinical response, attaining clinical response or remission, or treatment failure rate for patients treated with combination antibiotics, metronidazole monotherapy, or SOC. However, results of this study suggest that the use of combination antibiotics plus SOC may lead to a faster time to clinical response and remission compared to SOC therapy alone. Further studies are warranted to elucidate the role of antimicrobial therapy in management of pediatric IBD.</p>","PeriodicalId":45251,"journal":{"name":"Pediatric Reports","volume":"17 4","pages":""},"PeriodicalIF":1.4000,"publicationDate":"2025-07-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12286285/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/pediatric17040077","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
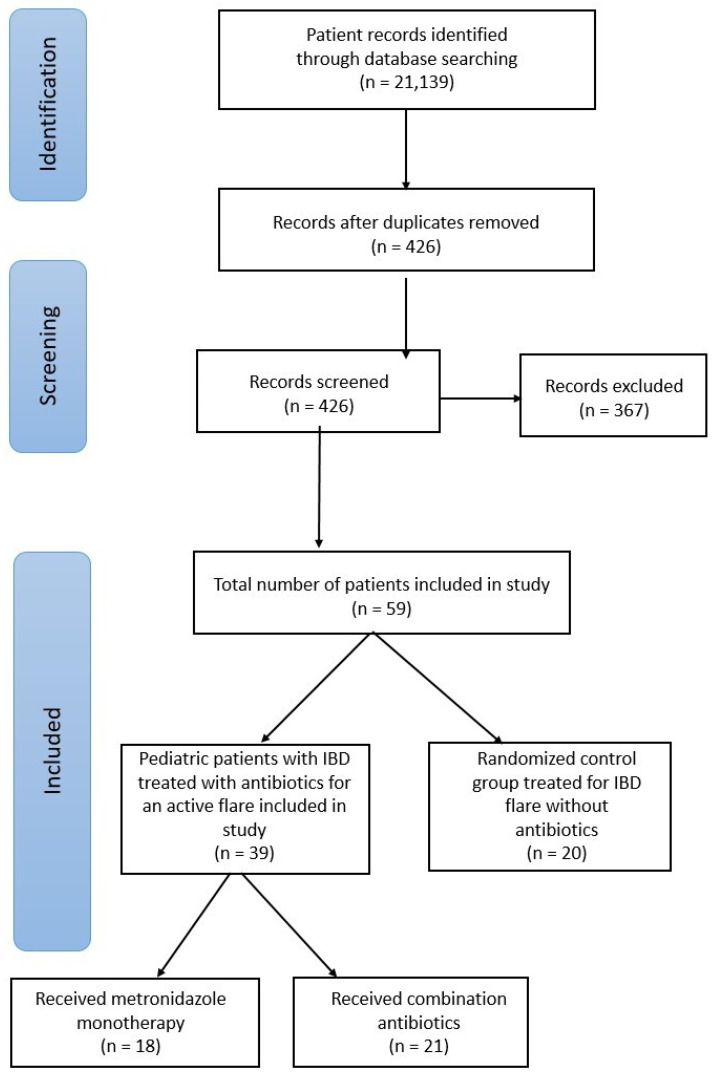
Objective: Gut dysbiosis has been implicated in the pathology of inflammatory bowel disease (IBD). There is some evidence to suggest that the use of antibiotic treatment can incite an early clinical response or remission when used in conjunction with standard-of-care (SOC) therapy to treat IBD-related flares. Furthermore, antibiotics have been historically investigated for use as a bridge when initiating biologic therapy while waiting for peak biologic treatment effect to occur. This study investigated and compared the time to clinical response when treated with combination antibiotics, metronidazole monotherapy, or SOC therapy in pediatric patients with an active IBD flare. Methods: This study was a retrospective, Institution Review Board-approved, single-centered cohort study which included patients who were less than 18 years of age with a confirmed diagnosis of IBD who received conventional treatment alone or with either combination antibiotic therapy or metronidazole monotherapy to treat an active IBD flare between March 2013 and January 2024. Patients were excluded if they received antibiotic therapy to treat an active infection, had positive stool cultures or enteric pathogen polymerase chain reaction panel, or had colonic disease limited to the rectum. Results: Fifty-nine patients were included and divided into metronidazole monotherapy (n = 18), SOC therapy (n = 20), and combination antibiotics (n = 21). The primary outcome of days to clinical response was not significantly different across all groups; however, patients who received combination antibiotics achieved the fastest time to clinical response (median (IRQ))-4 days (1, 65), compared to 7.5 days (1, 119) for the SOC group and 9 days (2, 217) for the metronidazole group. Secondary outcomes of achievement of clinical response, remission, or failure were determined to be non-significant between all groups. Conclusions: There is no significant difference in time to clinical response, attaining clinical response or remission, or treatment failure rate for patients treated with combination antibiotics, metronidazole monotherapy, or SOC. However, results of this study suggest that the use of combination antibiotics plus SOC may lead to a faster time to clinical response and remission compared to SOC therapy alone. Further studies are warranted to elucidate the role of antimicrobial therapy in management of pediatric IBD.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


