Severe Rectal Syphilis in the Setting of Profound HIV Immunosuppression: A Case Report Highlighting ERG/CD38 Immunophenotyping and a Review of the Literature.
Diana Marcela Carmona Valencia, Juan Diego López, Shirley Vanessa Correa Forero, Diana Marcela Bonilla Bonilla, Jorge Karim Assis, Yamil Liscano
{"title":"Severe Rectal Syphilis in the Setting of Profound HIV Immunosuppression: A Case Report Highlighting ERG/CD38 Immunophenotyping and a Review of the Literature.","authors":"Diana Marcela Carmona Valencia, Juan Diego López, Shirley Vanessa Correa Forero, Diana Marcela Bonilla Bonilla, Jorge Karim Assis, Yamil Liscano","doi":"10.3390/idr17040085","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background and Aim:</b> Syphilis, caused by <i>Treponema pallidum</i>, classically presents with genital or anal chancres; rectal involvement is rare and frequently misdiagnosed as inflammatory bowel disease or malignancy. We describe an unusually severe case of syphilitic proctitis in the setting of advanced HIV-related immunosuppression (CD4 39 cells/µL), in which targeted immunophenotyping (ERG and CD38) was a valuable adjunctive tool in the differential diagnosis. <b>Case Presentation:</b> A 46-year-old man with a recent history of erosive gastritis and esophageal candidiasis presented after six months of unintentional 20 kg weight loss, profound fatigue, intermittent fevers, profuse diarrhea, and two episodes of hematemesis. Workup revealed a new diagnosis of HIV infection (CD4: 39 cells/µL; viral load: 87,837 copies/mL). Contrast-enhanced CT demonstrated uniform, concentric rectal wall thickening (\"target sign\"). Colonoscopic biopsy showed exuberant granulation tissue and dense plasma cell infiltrates. Immunohistochemistry revealed a dense infiltrate of CD38-positive plasma cells and ERG-positive endothelial proliferation. These findings, in the context of positive serology, were highly supportive of a spirochetal etiology and helped differentiate it from potential mimics. Serology was positive for latent late syphilis (VDRL 1:64). The patient received three weekly doses of intramuscular benzathine penicillin; lumbar puncture excluded neurosyphilis. <b>Discussion:</b> This is among the first reported cases of syphilitic proctitis in a patient with CD4 < 50 cells/µL, where advanced immunophenotyping differentiated syphilitic inflammation from neoplastic or inflammatory mimics. Profound immunosuppression accelerates disease progression and yields atypical clinical features. <b>Conclusion:</b> In HIV-infected patients with chronic rectal symptoms, especially those with CD4 < 50 cells/µL, syphilitic proctitis must be considered. Integration of radiologic assessment, histopathology with ERG/CD38 staining, and serologic testing permits prompt diagnosis. Early benzathine penicillin therapy and rigorous clinical and serologic follow-up are essential to prevent complications, including neurosyphilis.</p>","PeriodicalId":13579,"journal":{"name":"Infectious Disease Reports","volume":"17 4","pages":""},"PeriodicalIF":2.4000,"publicationDate":"2025-07-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12286282/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Infectious Disease Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/idr17040085","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
Abstract
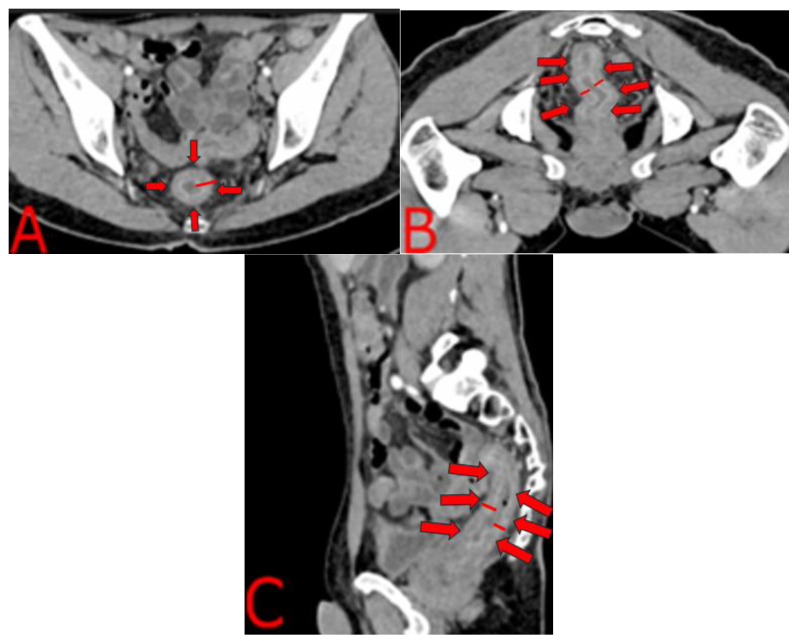
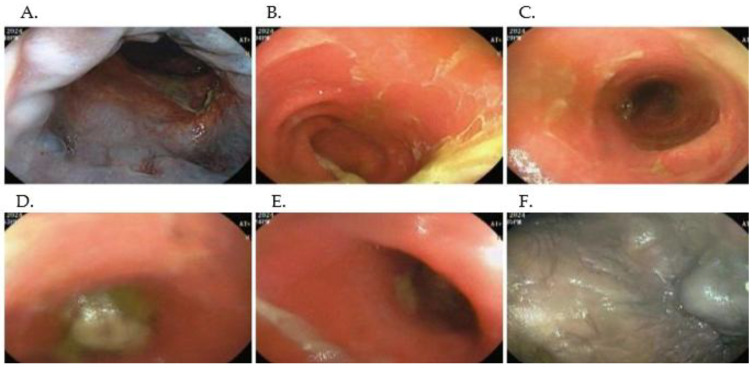
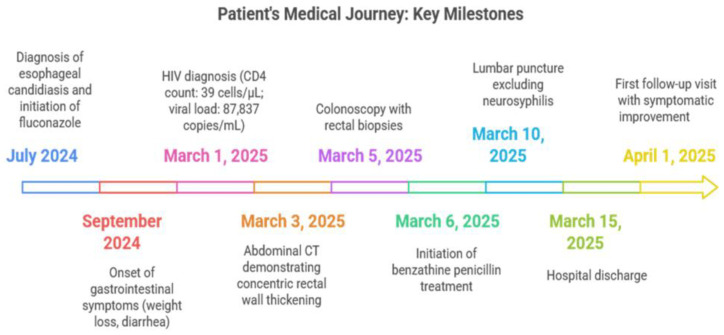
Background and Aim: Syphilis, caused by Treponema pallidum, classically presents with genital or anal chancres; rectal involvement is rare and frequently misdiagnosed as inflammatory bowel disease or malignancy. We describe an unusually severe case of syphilitic proctitis in the setting of advanced HIV-related immunosuppression (CD4 39 cells/µL), in which targeted immunophenotyping (ERG and CD38) was a valuable adjunctive tool in the differential diagnosis. Case Presentation: A 46-year-old man with a recent history of erosive gastritis and esophageal candidiasis presented after six months of unintentional 20 kg weight loss, profound fatigue, intermittent fevers, profuse diarrhea, and two episodes of hematemesis. Workup revealed a new diagnosis of HIV infection (CD4: 39 cells/µL; viral load: 87,837 copies/mL). Contrast-enhanced CT demonstrated uniform, concentric rectal wall thickening ("target sign"). Colonoscopic biopsy showed exuberant granulation tissue and dense plasma cell infiltrates. Immunohistochemistry revealed a dense infiltrate of CD38-positive plasma cells and ERG-positive endothelial proliferation. These findings, in the context of positive serology, were highly supportive of a spirochetal etiology and helped differentiate it from potential mimics. Serology was positive for latent late syphilis (VDRL 1:64). The patient received three weekly doses of intramuscular benzathine penicillin; lumbar puncture excluded neurosyphilis. Discussion: This is among the first reported cases of syphilitic proctitis in a patient with CD4 < 50 cells/µL, where advanced immunophenotyping differentiated syphilitic inflammation from neoplastic or inflammatory mimics. Profound immunosuppression accelerates disease progression and yields atypical clinical features. Conclusion: In HIV-infected patients with chronic rectal symptoms, especially those with CD4 < 50 cells/µL, syphilitic proctitis must be considered. Integration of radiologic assessment, histopathology with ERG/CD38 staining, and serologic testing permits prompt diagnosis. Early benzathine penicillin therapy and rigorous clinical and serologic follow-up are essential to prevent complications, including neurosyphilis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


