Nisha George, Daniel Pan, Shirley Sze, Caroline Williams, Zein El-Dean, Victor Zlocha, Elizabeth Webb, Manish Pareek
{"title":"Gummatous mitral valve endocarditis from tertiary syphilis.","authors":"Nisha George, Daniel Pan, Shirley Sze, Caroline Williams, Zein El-Dean, Victor Zlocha, Elizabeth Webb, Manish Pareek","doi":"10.1099/acmi.0.000817.v3","DOIUrl":null,"url":null,"abstract":"<p><p>A 50-year-old Romanian gentleman presented with fever, myalgia and 30 kg weight loss. He was treated for syphilis after acquiring it 16 years ago. On examination, there was a pansystolic murmur in the axilla, and the patient had an ataxic gait. Blood tests showed raised inflammatory markers. However, standard investigations for infective endocarditis, including multiple blood cultures, serological titres for fastidious organisms and antibody tests were negative. A computed tomography (CT) of the chest, abdomen and pelvis demonstrated hepatosplenomegaly with multiple splenic infarcts. A magnetic resonance imaging (MRI) of the head with contrast showed multiple punctate enhancement in the bilateral hemispheres with leptomeningeal enhancement. Transthoracic echocardiogram demonstrated a large vegetation leading to severe mitral regurgitation. Serum treponemal antibodies were positive; <i>Treponema pallidum</i> particle agglutination (TPPA) was positive at 1 : 1280, and rapid plasma reagin (RPR) 1 : 4 treponemal IgM was negative; lumbar puncture syphilis serology was negative. The patient was treated with an extensive period of intravenous antibiotics, in addition to a prosthetic metallic valve replacement, where unusual ragged calcified valvular tissue was observed. Tertiary syphilis is a difficult diagnosis to confirm, since it can often be indolent and occur in areas of the body where it may go unnoticed. In our case, a diagnosis of probable syphilitic endocarditis was made from a combination of the history, an initial increase in the size of the lesion following antibiotic therapy and observation of likely gumma on the mitral valve during surgery. In such cases, surgery in addition to optimal antimicrobial therapy is necessary for effective treatment. This case adds to the current literature that treatment with penicillin is likely inadequate to prevent late complications.</p>","PeriodicalId":94366,"journal":{"name":"Access microbiology","volume":"7 5","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2025-05-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12281932/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Access microbiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1099/acmi.0.000817.v3","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
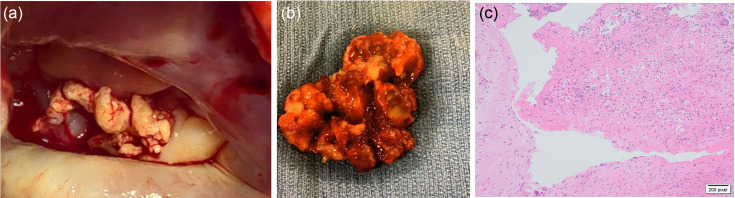
A 50-year-old Romanian gentleman presented with fever, myalgia and 30 kg weight loss. He was treated for syphilis after acquiring it 16 years ago. On examination, there was a pansystolic murmur in the axilla, and the patient had an ataxic gait. Blood tests showed raised inflammatory markers. However, standard investigations for infective endocarditis, including multiple blood cultures, serological titres for fastidious organisms and antibody tests were negative. A computed tomography (CT) of the chest, abdomen and pelvis demonstrated hepatosplenomegaly with multiple splenic infarcts. A magnetic resonance imaging (MRI) of the head with contrast showed multiple punctate enhancement in the bilateral hemispheres with leptomeningeal enhancement. Transthoracic echocardiogram demonstrated a large vegetation leading to severe mitral regurgitation. Serum treponemal antibodies were positive; Treponema pallidum particle agglutination (TPPA) was positive at 1 : 1280, and rapid plasma reagin (RPR) 1 : 4 treponemal IgM was negative; lumbar puncture syphilis serology was negative. The patient was treated with an extensive period of intravenous antibiotics, in addition to a prosthetic metallic valve replacement, where unusual ragged calcified valvular tissue was observed. Tertiary syphilis is a difficult diagnosis to confirm, since it can often be indolent and occur in areas of the body where it may go unnoticed. In our case, a diagnosis of probable syphilitic endocarditis was made from a combination of the history, an initial increase in the size of the lesion following antibiotic therapy and observation of likely gumma on the mitral valve during surgery. In such cases, surgery in addition to optimal antimicrobial therapy is necessary for effective treatment. This case adds to the current literature that treatment with penicillin is likely inadequate to prevent late complications.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


