[Recommendations from an antimicrobial stewardship program on the duration of antibiotic treatment: effectiveness of short-course regimens in the emergency department].
Paula Martínez-de La Cruz, Sira Sánz-Márquez, José Francisco Valverde-Cánovas, Rafael Hervás-Gómez, Oriol Martín-Segarra, Ana Vegas-Serrano, María Velasco-Arribas, Juan Emilio Losa-García, Leonor Moreno-Núñez
{"title":"[Recommendations from an antimicrobial stewardship program on the duration of antibiotic treatment: effectiveness of short-course regimens in the emergency department].","authors":"Paula Martínez-de La Cruz, Sira Sánz-Márquez, José Francisco Valverde-Cánovas, Rafael Hervás-Gómez, Oriol Martín-Segarra, Ana Vegas-Serrano, María Velasco-Arribas, Juan Emilio Losa-García, Leonor Moreno-Núñez","doi":"10.37201/req/040.2025","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Excessive duration of antibiotic treatment is associated with adverse events without improving clinical outcomes. The Emergency Department (ED) is a strategic location to implement Antibiotic Stewardship Programs (ASP). Our objective was to determine the effect of ASP recommendations on short antibiotic treatment regimens in patients with uncomplicated infections treated in the ED.</p><p><strong>Material and methods: </strong>We conducted a quasi-experimental study comparing patients treated in the ED in September and October 2022 who were discharged with antibiotic treatment (control group) with those treated in November and December of the same year (intervention group). Recommendations regarding the appropriateness of antibiotic therapy were made in both groups, and regarding treatment duration only in the intervention group. A 30-day follow-up was performed to assess healing, readmissions due to infection, and adverse effects.</p><p><strong>Results: </strong>A total of 78 patients were included, 40 in the control group and 38 in the intervention group. The median duration of antibiotic treatment was significantly shorter in the intervention group (7.5 days, IQR: 7-10 vs 6 days, IQR: 5-7, p<0.001). Healing rates were similar in both groups (92.5% vs 97.4%, p = 0.616). Adverse effects were documented in 7 patients from the intervention group (18.4%).</p><p><strong>Conclusions: </strong>An ASP in the ED can shorten the duration of antibiotic treatment in patients with uncomplicated infections who are discharged, without affecting clinical outcomes, and without being associated with severe adverse effects, mortality, or readmissions due to infection.</p>","PeriodicalId":94198,"journal":{"name":"Revista espanola de quimioterapia : publicacion oficial de la Sociedad Espanola de Quimioterapia","volume":" ","pages":"420-425"},"PeriodicalIF":2.2000,"publicationDate":"2025-09-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12447301/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Revista espanola de quimioterapia : publicacion oficial de la Sociedad Espanola de Quimioterapia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.37201/req/040.2025","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/23 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Excessive duration of antibiotic treatment is associated with adverse events without improving clinical outcomes. The Emergency Department (ED) is a strategic location to implement Antibiotic Stewardship Programs (ASP). Our objective was to determine the effect of ASP recommendations on short antibiotic treatment regimens in patients with uncomplicated infections treated in the ED.
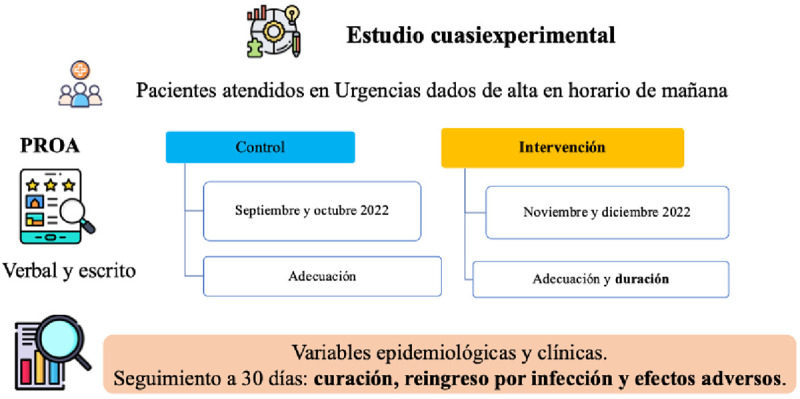
Material and methods: We conducted a quasi-experimental study comparing patients treated in the ED in September and October 2022 who were discharged with antibiotic treatment (control group) with those treated in November and December of the same year (intervention group). Recommendations regarding the appropriateness of antibiotic therapy were made in both groups, and regarding treatment duration only in the intervention group. A 30-day follow-up was performed to assess healing, readmissions due to infection, and adverse effects.
Results: A total of 78 patients were included, 40 in the control group and 38 in the intervention group. The median duration of antibiotic treatment was significantly shorter in the intervention group (7.5 days, IQR: 7-10 vs 6 days, IQR: 5-7, p<0.001). Healing rates were similar in both groups (92.5% vs 97.4%, p = 0.616). Adverse effects were documented in 7 patients from the intervention group (18.4%).
Conclusions: An ASP in the ED can shorten the duration of antibiotic treatment in patients with uncomplicated infections who are discharged, without affecting clinical outcomes, and without being associated with severe adverse effects, mortality, or readmissions due to infection.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


