Véronique Déry, Gabrielle Lafond, Rosemarie Picard, Pierre Langevin
{"title":"Recovery from Mild Traumatic Brain Injury in the Nonathletic Population: A Systematic Review.","authors":"Véronique Déry, Gabrielle Lafond, Rosemarie Picard, Pierre Langevin","doi":"10.1089/neur.2025.0006","DOIUrl":null,"url":null,"abstract":"<p><p>The objective of this study was to document the resolution rate of mild Traumatic Brain Injury (mTBI) symptoms at various time points in a nonathletic adult population and identify prognostic factors influencing recovery. Sixteen prospective cohort studies were included, focusing on participants aged 18-65 with acute mTBI, followed for a minimum of 1 month. The recovery criterion was the resolution of symptoms not attributable to pre-existing conditions. Risk of bias was assessed using the Quality in Prognostic Studies tool, with most studies rated as moderate risk, highlighting variability in methodological rigor. Symptom resolution was reported in 49.0% to 69.5% of patients at 1 month, 40.8% to 84.4% at 3 months, 38.3% to 72.2% at 6 months, and 58.1 to 68.3% at 12 months. These findings emphasize the first 6 months as a critical period for evaluating the risk of symptom chronicity. The most commonly reported prognostic factors was baseline symptom severity, including higher intensity of symptoms such as headaches, nausea, and dizziness, as well as elevated scores on validated symptom scales. Psychiatric history, such as pre-existing anxiety or depression, was also a significant predictor of prolonged symptoms. Biomarkers, including NSE and S-100B levels, and reduced blood-derived neurotrophic factors, were associated with poorer recovery at 6 months. Demographic factors, including age, gender, and education level, showed mixed results. While some studies associated female gender, older age, and lower education with poorer recovery, others found no significant correlations. These discrepancies highlight the complexity of mTBI prognosis. Overall, more than half of patients recover within 6 months, but persistent symptoms can have a profound impact on quality of life and functional status. Identifying patients at higher risk of prolonged recovery is crucial for targeted management strategies, emphasizing the importance of individualized, evidence-based care in mTBI populations.</p>","PeriodicalId":74300,"journal":{"name":"Neurotrauma reports","volume":"6 1","pages":"355-374"},"PeriodicalIF":1.8000,"publicationDate":"2025-04-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12281108/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurotrauma reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1089/neur.2025.0006","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
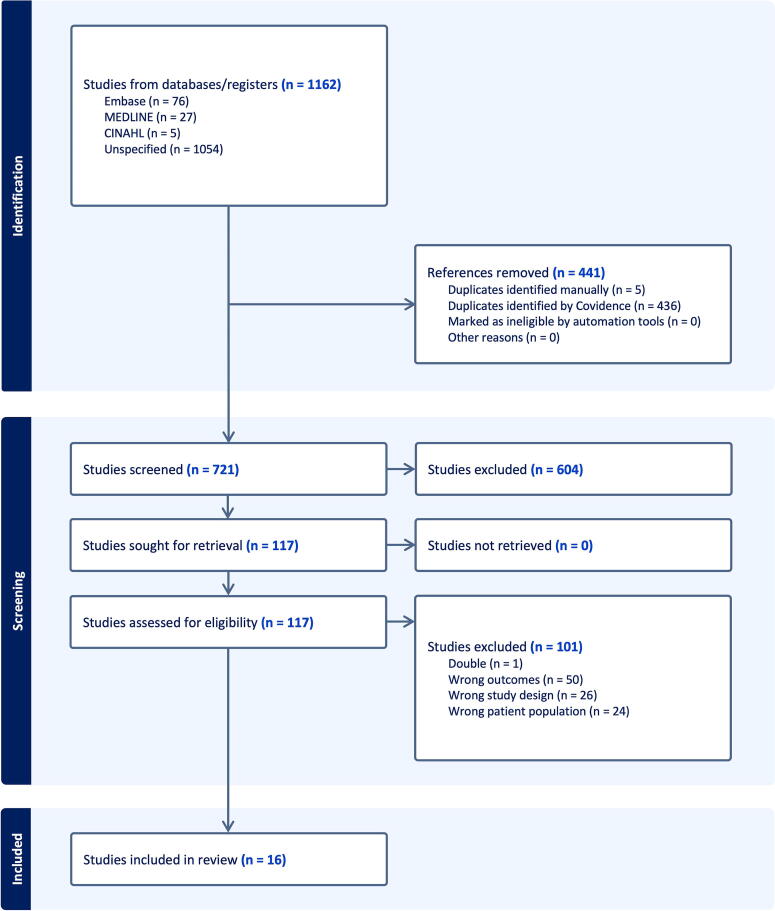
The objective of this study was to document the resolution rate of mild Traumatic Brain Injury (mTBI) symptoms at various time points in a nonathletic adult population and identify prognostic factors influencing recovery. Sixteen prospective cohort studies were included, focusing on participants aged 18-65 with acute mTBI, followed for a minimum of 1 month. The recovery criterion was the resolution of symptoms not attributable to pre-existing conditions. Risk of bias was assessed using the Quality in Prognostic Studies tool, with most studies rated as moderate risk, highlighting variability in methodological rigor. Symptom resolution was reported in 49.0% to 69.5% of patients at 1 month, 40.8% to 84.4% at 3 months, 38.3% to 72.2% at 6 months, and 58.1 to 68.3% at 12 months. These findings emphasize the first 6 months as a critical period for evaluating the risk of symptom chronicity. The most commonly reported prognostic factors was baseline symptom severity, including higher intensity of symptoms such as headaches, nausea, and dizziness, as well as elevated scores on validated symptom scales. Psychiatric history, such as pre-existing anxiety or depression, was also a significant predictor of prolonged symptoms. Biomarkers, including NSE and S-100B levels, and reduced blood-derived neurotrophic factors, were associated with poorer recovery at 6 months. Demographic factors, including age, gender, and education level, showed mixed results. While some studies associated female gender, older age, and lower education with poorer recovery, others found no significant correlations. These discrepancies highlight the complexity of mTBI prognosis. Overall, more than half of patients recover within 6 months, but persistent symptoms can have a profound impact on quality of life and functional status. Identifying patients at higher risk of prolonged recovery is crucial for targeted management strategies, emphasizing the importance of individualized, evidence-based care in mTBI populations.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


