Disease activity at two consecutive registry visits and subsequent medication escalation for patients with juvenile idiopathic arthritis in the CARRA registry.
Melissa L Mannion, Monica S Aswani, K Ria Hearld, Emily A Smitherman, Livie Timmerman, Jeffrey R Curtis
{"title":"Disease activity at two consecutive registry visits and subsequent medication escalation for patients with juvenile idiopathic arthritis in the CARRA registry.","authors":"Melissa L Mannion, Monica S Aswani, K Ria Hearld, Emily A Smitherman, Livie Timmerman, Jeffrey R Curtis","doi":"10.1186/s12969-025-01130-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To account for the chronic time course of juvenile idiopathic arthritis (JIA), we assessed medication changes by disease activity patterns across 2 sequential timepoints.</p><p><strong>Methods: </strong>Patients with non-systemic JIA enrolled in the Childhood Arthritis and Rheumatology Research Alliance Registry with complete clinical Juvenile Arthritis Disease Activity Scores (cJADAS) at 6 and 12-month registry visits were included. Disease activity was classified by cJADAS categories (inactive/minimal, moderate/high). The primary outcome was disease modifying anti-rheumatic drug (DMARD) escalation at the 12-month visit. We examined the association between cJADAS patterns and DMARD escalation.</p><p><strong>Results: </strong>The cJADAS patterns across paired visits for 2,956 patients with JIA were: 71% persistent inactive/minimal, 25% persistent moderate/high, 2% \"improving\", and 2% \"flaring\". Only 10% of patients had DMARD escalation at the 12-month visit, including only 15% of patients with persistent moderate/high disease activity. In multivariable logistic regression adjusting for sociodemographic and clinical variables, DMARD escalation at the 12-month visit was associated with \"flaring\" disease activity (odds ratio [OR] 2.62, 95% confidence interval [CI] 1.33-5.18), DMARD escalation between the 6- and 12-month visits (OR 1.86, 95% CI 1.40-2.49) and morning stiffness (> 60 min 4.98, 95% CI 3.00-8.27), while age 15-19 years were less likely to escalate (OR 0.61, 95% CI 0.38-0.97).</p><p><strong>Conclusion: </strong>In a large multicenter registry of US patients with JIA, DMARD escalation at the 12-month visit was uncommon overall, even for those with persistent moderate/high disease activity. Our findings suggest that DMARD escalation in this cohort did not align well with a treat to target approach using cJADAS thresholds.</p>","PeriodicalId":54630,"journal":{"name":"Pediatric Rheumatology","volume":"23 1","pages":"77"},"PeriodicalIF":2.3000,"publicationDate":"2025-07-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12285171/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric Rheumatology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12969-025-01130-2","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: To account for the chronic time course of juvenile idiopathic arthritis (JIA), we assessed medication changes by disease activity patterns across 2 sequential timepoints.
Methods: Patients with non-systemic JIA enrolled in the Childhood Arthritis and Rheumatology Research Alliance Registry with complete clinical Juvenile Arthritis Disease Activity Scores (cJADAS) at 6 and 12-month registry visits were included. Disease activity was classified by cJADAS categories (inactive/minimal, moderate/high). The primary outcome was disease modifying anti-rheumatic drug (DMARD) escalation at the 12-month visit. We examined the association between cJADAS patterns and DMARD escalation.
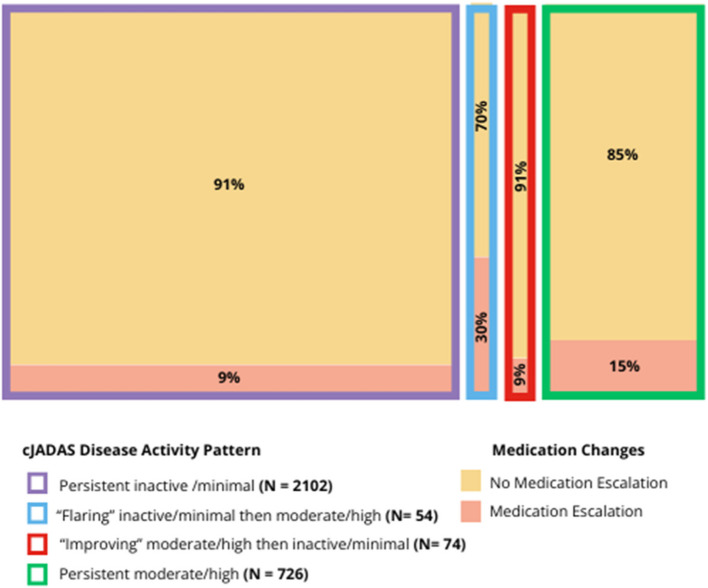
Results: The cJADAS patterns across paired visits for 2,956 patients with JIA were: 71% persistent inactive/minimal, 25% persistent moderate/high, 2% "improving", and 2% "flaring". Only 10% of patients had DMARD escalation at the 12-month visit, including only 15% of patients with persistent moderate/high disease activity. In multivariable logistic regression adjusting for sociodemographic and clinical variables, DMARD escalation at the 12-month visit was associated with "flaring" disease activity (odds ratio [OR] 2.62, 95% confidence interval [CI] 1.33-5.18), DMARD escalation between the 6- and 12-month visits (OR 1.86, 95% CI 1.40-2.49) and morning stiffness (> 60 min 4.98, 95% CI 3.00-8.27), while age 15-19 years were less likely to escalate (OR 0.61, 95% CI 0.38-0.97).
Conclusion: In a large multicenter registry of US patients with JIA, DMARD escalation at the 12-month visit was uncommon overall, even for those with persistent moderate/high disease activity. Our findings suggest that DMARD escalation in this cohort did not align well with a treat to target approach using cJADAS thresholds.
目的:为了解释青少年特发性关节炎(JIA)的慢性病程,我们通过2个连续时间点的疾病活动模式来评估药物变化。方法:纳入儿童关节炎和风湿病研究联盟注册的非全身性JIA患者,这些患者在6个月和12个月的注册访问中具有完整的临床幼年关节炎疾病活动评分(cJADAS)。疾病活动性按cJADAS分类(无活性/轻度、中度/高度)进行分类。主要终点是12个月随访时疾病改善抗风湿药物(DMARD)的升级。我们研究了cJADAS模式与DMARD升级之间的关系。结果:2956例JIA患者的cJADAS模式为:71%持续不活跃/轻度,25%持续中度/重度,2%“改善”,2%“恶化”。在12个月的随访中,只有10%的患者DMARD升级,其中只有15%的患者持续中/高疾病活动性。在调整社会人口学和临床变量的多变量logistic回归中,12个月就诊时DMARD升级与“爆发”疾病活动(优势比[OR] 2.62, 95%可信区间[CI] 1.33-5.18)、6个月和12个月就诊时DMARD升级(OR 1.86, 95% CI 1.40-2.49)和晨僵(bbb60分钟4.98,95% CI 3.00-8.27)相关,而15-19岁患者升级的可能性较小(OR 0.61, 95% CI 0.38-0.97)。结论:在美国JIA患者的大型多中心登记中,在12个月的随访中,DMARD升级总体上是罕见的,即使对于那些持续中/高疾病活动度的患者也是如此。我们的研究结果表明,该队列中的DMARD升级与使用cJADAS阈值的治疗到靶点方法不一致。
期刊介绍:
Pediatric Rheumatology is an open access, peer-reviewed, online journal encompassing all aspects of clinical and basic research related to pediatric rheumatology and allied subjects.
The journal’s scope of diseases and syndromes include musculoskeletal pain syndromes, rheumatic fever and post-streptococcal syndromes, juvenile idiopathic arthritis, systemic lupus erythematosus, juvenile dermatomyositis, local and systemic scleroderma, Kawasaki disease, Henoch-Schonlein purpura and other vasculitides, sarcoidosis, inherited musculoskeletal syndromes, autoinflammatory syndromes, and others.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


