Patient barriers and facilitators to lung cancer screening uptake and intention to screen: a systematic review using the Theoretical Domains Framework.
Maira Salman, Alice Cotton, Ada Humphrey, Tania Domun, Calvin Cheng, Gaby Judah
{"title":"Patient barriers and facilitators to lung cancer screening uptake and intention to screen: a systematic review using the Theoretical Domains Framework.","authors":"Maira Salman, Alice Cotton, Ada Humphrey, Tania Domun, Calvin Cheng, Gaby Judah","doi":"10.1136/bmjresp-2024-003127","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Lung cancer is the leading cause of cancer deaths worldwide. Screening high-risk individuals with low-dose CT (LDCT) reduces mortality through earlier detection, when treatment may be curable. In countries where formal screening programmes exist, uptake among eligible populations remains low. Understanding barriers to uptake could help identify interventions to support attendance.</p><p><strong>Aim: </strong>To identify barriers and facilitators to intention to screen and uptake of LDCT as a form of lung cancer screening, from a review of existing literature.</p><p><strong>Method: </strong>Three databases were used along with a grey literature search. Inclusion criteria were studied: published in English between 2001 and 2024; looking at patient-reported psychological barriers and facilitators and related to uptake (including intent to uptake) of first LDCT as method of lung cancer screening. Determinants were extracted from the papers, and whether these were reported as a barrier, facilitator or both. Determinants were then mapped to the Theoretical Domains Framework (TDF) domains to classify determinants using a theory-based approach.</p><p><strong>Results: </strong>From an initial 2491 results, 72 papers were included (67% explored intention to screen), which reported 34 variables covering 10 TDF domains. Fear (of either lung cancer diagnosis due to fatalism (22 studies) or of screening procedure (13)), categorised in TDF domain Emotion, was the most frequently reported barrier followed by Environmental Context and Resource barriers of cost of procedure (28), inconvenience of attending (24) and lack of knowledge (24) (TDF: Knowledge). Most frequently identified facilitators were clinician recommendation (26) (TDF: Social Influence) and perceived personal benefit from attending screening (25) (TDF: Beliefs about Consequences).</p><p><strong>Conclusion: </strong>To increase uptake in screening, interventions addressing these determinants should be designed and tested. These could include interventions to mitigate fear of screening, reduce the costs of attending and promote clinician endorsement.</p>","PeriodicalId":9048,"journal":{"name":"BMJ Open Respiratory Research","volume":"12 1","pages":""},"PeriodicalIF":3.4000,"publicationDate":"2025-07-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12281332/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Open Respiratory Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/bmjresp-2024-003127","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Lung cancer is the leading cause of cancer deaths worldwide. Screening high-risk individuals with low-dose CT (LDCT) reduces mortality through earlier detection, when treatment may be curable. In countries where formal screening programmes exist, uptake among eligible populations remains low. Understanding barriers to uptake could help identify interventions to support attendance.
Aim: To identify barriers and facilitators to intention to screen and uptake of LDCT as a form of lung cancer screening, from a review of existing literature.
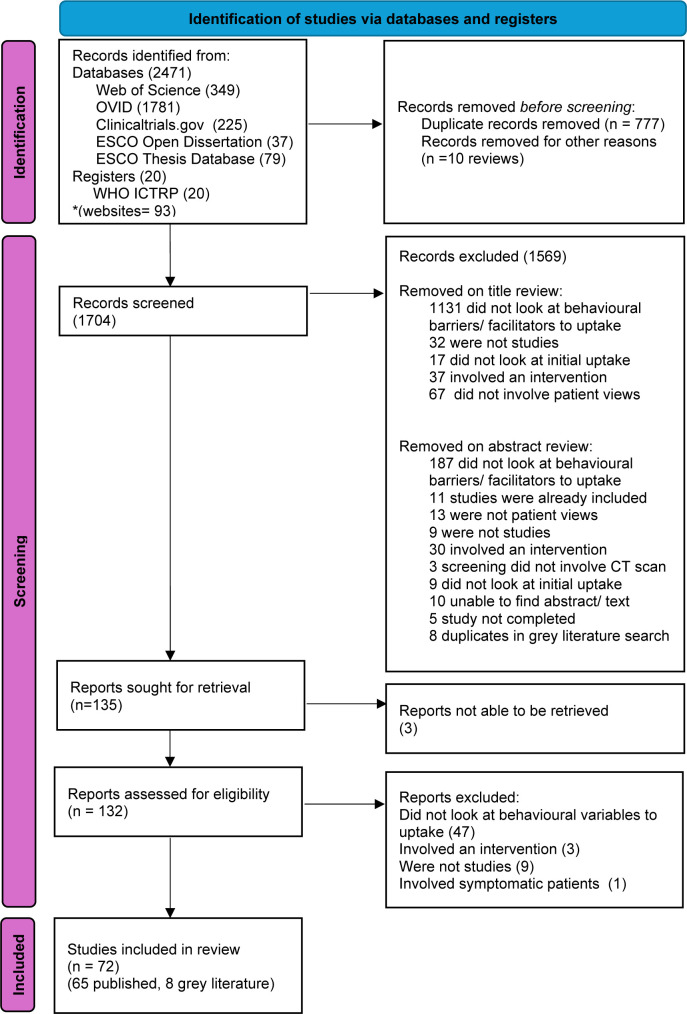
Method: Three databases were used along with a grey literature search. Inclusion criteria were studied: published in English between 2001 and 2024; looking at patient-reported psychological barriers and facilitators and related to uptake (including intent to uptake) of first LDCT as method of lung cancer screening. Determinants were extracted from the papers, and whether these were reported as a barrier, facilitator or both. Determinants were then mapped to the Theoretical Domains Framework (TDF) domains to classify determinants using a theory-based approach.
Results: From an initial 2491 results, 72 papers were included (67% explored intention to screen), which reported 34 variables covering 10 TDF domains. Fear (of either lung cancer diagnosis due to fatalism (22 studies) or of screening procedure (13)), categorised in TDF domain Emotion, was the most frequently reported barrier followed by Environmental Context and Resource barriers of cost of procedure (28), inconvenience of attending (24) and lack of knowledge (24) (TDF: Knowledge). Most frequently identified facilitators were clinician recommendation (26) (TDF: Social Influence) and perceived personal benefit from attending screening (25) (TDF: Beliefs about Consequences).
Conclusion: To increase uptake in screening, interventions addressing these determinants should be designed and tested. These could include interventions to mitigate fear of screening, reduce the costs of attending and promote clinician endorsement.
期刊介绍:
BMJ Open Respiratory Research is a peer-reviewed, open access journal publishing respiratory and critical care medicine. It is the sister journal to Thorax and co-owned by the British Thoracic Society and BMJ. The journal focuses on robustness of methodology and scientific rigour with less emphasis on novelty or perceived impact. BMJ Open Respiratory Research operates a rapid review process, with continuous publication online, ensuring timely, up-to-date research is available worldwide. The journal publishes review articles and all research study types: Basic science including laboratory based experiments and animal models, Pilot studies or proof of concept, Observational studies, Study protocols, Registries, Clinical trials from phase I to multicentre randomised clinical trials, Systematic reviews and meta-analyses.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


