Carline N L Groenland, Matthijs L Janssen, Kim S van den Bosch, Vivan J M Baggen, Leo Heunks, Henrik Endeman, Evert-Jan Wils
{"title":"Liberation from invasive mechanical ventilation: a nationwide survey among intensive care units in the Netherlands.","authors":"Carline N L Groenland, Matthijs L Janssen, Kim S van den Bosch, Vivan J M Baggen, Leo Heunks, Henrik Endeman, Evert-Jan Wils","doi":"10.1136/bmjresp-2024-002868","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Liberation from invasive mechanical ventilation is a milestone in critical care, but approaches vary. This survey aimed to describe current ventilator liberation practices, relate them to available evidence, and identify areas for improvement.</p><p><strong>Methods: </strong>A survey was performed among Dutch intensive care unit (ICU) sites. The survey evaluated practice in seven domains of ventilator liberation: protocol availability, transition from controlled to assisted ventilation, spontaneous breathing trials (SBT), cuff-leak test, postextubation support, weaning failure and tracheostomised weaning.</p><p><strong>Results: </strong>The survey response rate was 93% (132/142), representing 97% (69/71) of Dutch ICUs. Protocols for postextubation support and weaning failure were available in less than half of the ICUs (44% and 49%, respectively). The transition from controlled to assisted ventilation is regularly evaluated daily in 78% of ICUs. Assisted ventilation tolerance is mainly assessed by clinical signs, respiratory parameters and non-invasive manoeuvres that assess respiratory drive (P<sub>0.1</sub>). SBTs are regularly performed in 58% of ICUs, using one or more of the following methods: T-piece (52%), pressure support+positive end expiratory pressure (32%) and continuous positive airway pressure (28%). Cuff-leak tests are seldom performed (1.4%), predominantly in cases of intubation for upper-airway obstruction (92%). Postextubation respiratory support with high-flow nasal oxygen or non-invasive ventilation is used at least as often with therapeutic (43%/13%) rather than preventive (35%/4%) of facilitative intent (29%/3%). Delirium screening (87%) and reconsidering sedation (84%) are frequently assessed in case of weaning failure. Regular use of closed-loop ventilation is reported in a minority of ICUs throughout the process of ventilator liberation (3-9%).</p><p><strong>Conclusions: </strong>Various aspects of ventilator liberation practices show only limited alignment with existing guidelines. The results of this survey pinpoint areas to prioritise in guideline and practice improvement.</p>","PeriodicalId":9048,"journal":{"name":"BMJ Open Respiratory Research","volume":"12 1","pages":""},"PeriodicalIF":3.4000,"publicationDate":"2025-07-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12281335/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Open Respiratory Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/bmjresp-2024-002868","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Liberation from invasive mechanical ventilation is a milestone in critical care, but approaches vary. This survey aimed to describe current ventilator liberation practices, relate them to available evidence, and identify areas for improvement.
Methods: A survey was performed among Dutch intensive care unit (ICU) sites. The survey evaluated practice in seven domains of ventilator liberation: protocol availability, transition from controlled to assisted ventilation, spontaneous breathing trials (SBT), cuff-leak test, postextubation support, weaning failure and tracheostomised weaning.
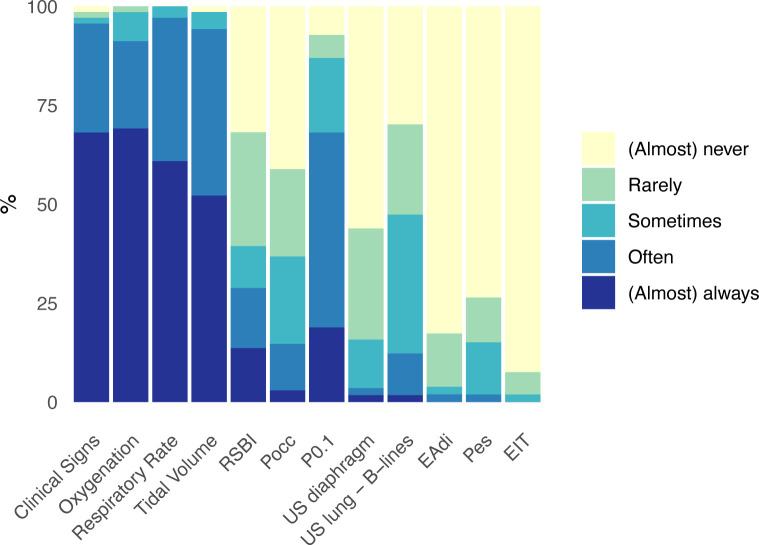
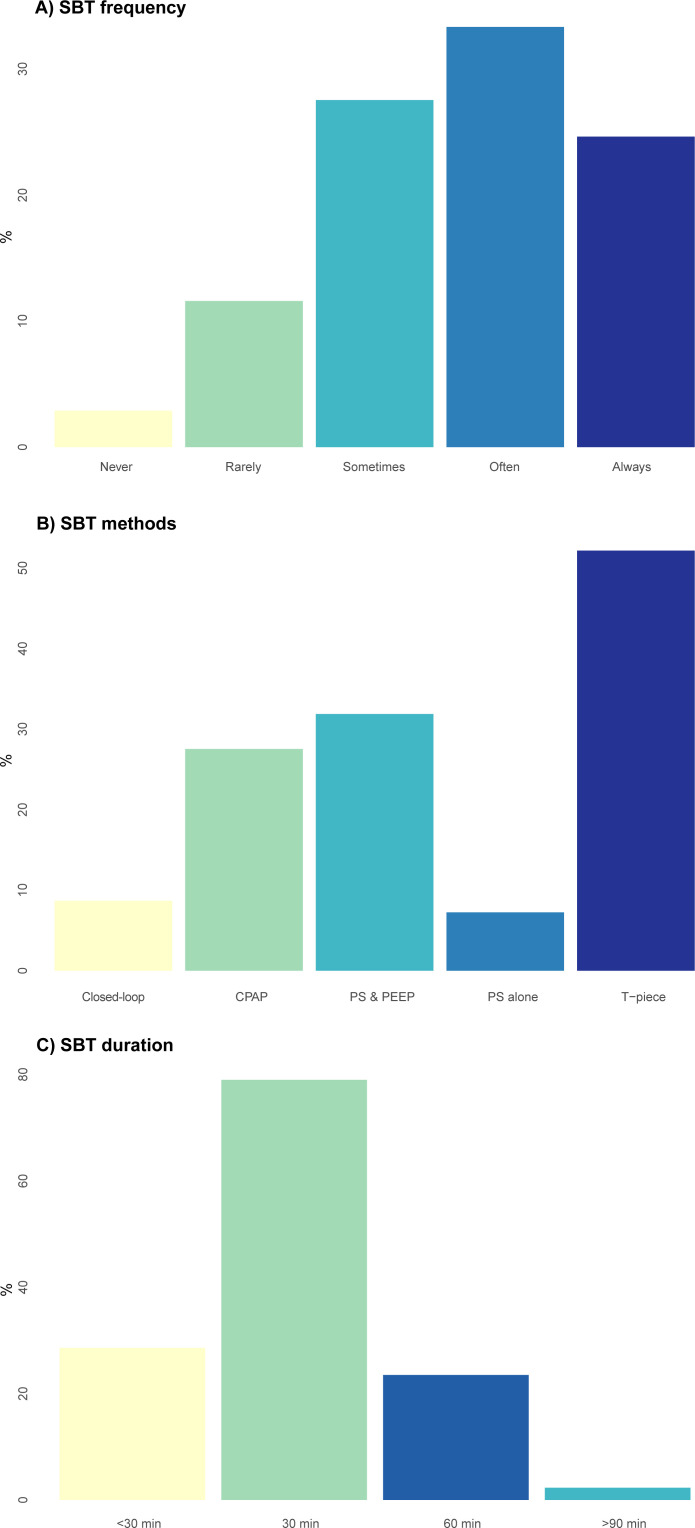
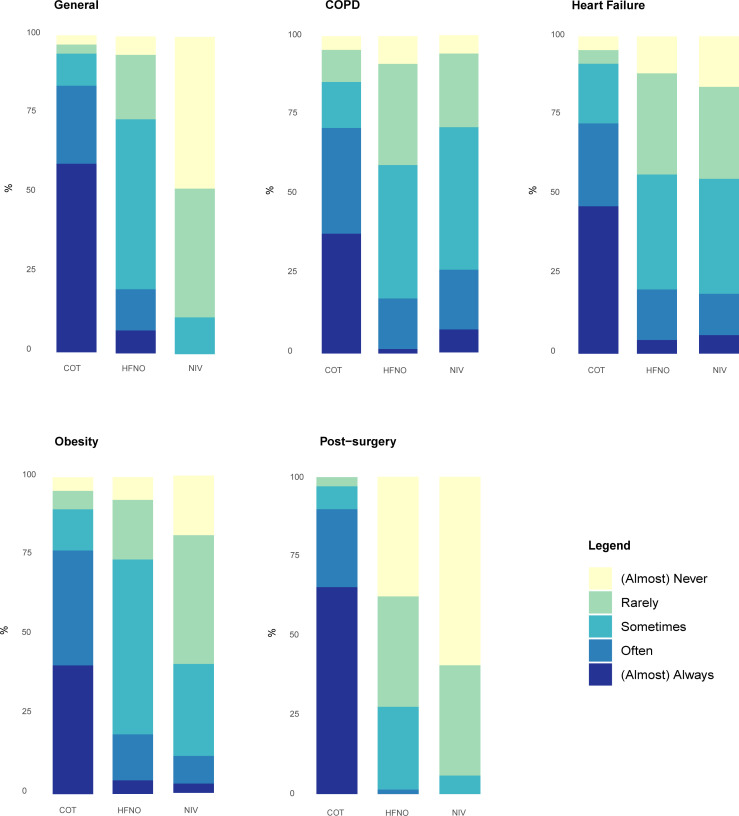
Results: The survey response rate was 93% (132/142), representing 97% (69/71) of Dutch ICUs. Protocols for postextubation support and weaning failure were available in less than half of the ICUs (44% and 49%, respectively). The transition from controlled to assisted ventilation is regularly evaluated daily in 78% of ICUs. Assisted ventilation tolerance is mainly assessed by clinical signs, respiratory parameters and non-invasive manoeuvres that assess respiratory drive (P0.1). SBTs are regularly performed in 58% of ICUs, using one or more of the following methods: T-piece (52%), pressure support+positive end expiratory pressure (32%) and continuous positive airway pressure (28%). Cuff-leak tests are seldom performed (1.4%), predominantly in cases of intubation for upper-airway obstruction (92%). Postextubation respiratory support with high-flow nasal oxygen or non-invasive ventilation is used at least as often with therapeutic (43%/13%) rather than preventive (35%/4%) of facilitative intent (29%/3%). Delirium screening (87%) and reconsidering sedation (84%) are frequently assessed in case of weaning failure. Regular use of closed-loop ventilation is reported in a minority of ICUs throughout the process of ventilator liberation (3-9%).
Conclusions: Various aspects of ventilator liberation practices show only limited alignment with existing guidelines. The results of this survey pinpoint areas to prioritise in guideline and practice improvement.
期刊介绍:
BMJ Open Respiratory Research is a peer-reviewed, open access journal publishing respiratory and critical care medicine. It is the sister journal to Thorax and co-owned by the British Thoracic Society and BMJ. The journal focuses on robustness of methodology and scientific rigour with less emphasis on novelty or perceived impact. BMJ Open Respiratory Research operates a rapid review process, with continuous publication online, ensuring timely, up-to-date research is available worldwide. The journal publishes review articles and all research study types: Basic science including laboratory based experiments and animal models, Pilot studies or proof of concept, Observational studies, Study protocols, Registries, Clinical trials from phase I to multicentre randomised clinical trials, Systematic reviews and meta-analyses.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


