Increased capture of post-endoscopic retrograde cholangiopancreatography adverse events by delayed (day 7) follow-up calls: a prospective comparison of physician- and nurse-initiated calls.
{"title":"Increased capture of post-endoscopic retrograde cholangiopancreatography adverse events by delayed (day 7) follow-up calls: a prospective comparison of physician- and nurse-initiated calls.","authors":"Monique T Barakat, Subhas Banerjee","doi":"10.20524/aog.2025.0970","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Endoscopic retrograde cholangiopancreatography (ERCP) is a high-risk endoscopic procedure. We recently found that physician-initiated post-ERCP follow-up calls on day 7 post-ERCP increased adverse event capture. Subsequently, we prospectively evaluated the utility of nurse-initiated follow-up calls, comparing these with physician-initiated calls to assess the impact of transitioning this responsibility to a nurse.</p><p><strong>Methods: </strong>This prospective study was conducted on consecutive patients undergoing ERCP at our academic tertiary care medical center. Patients received phone calls on days 1 and 7 post-ERCP, from either an endoscopist or a nurse coordinator, using a standardized script to assess delayed complications (pancreatitis, non-pancreatitis abdominal pain, bleeding, infection, perforation), and unplanned health encounters.</p><p><strong>Results: </strong>A total of 448 ERCP patients (239 physician calls, 209 nursing calls) were included. Physician calls were more successful than nursing calls in reaching patients on both day 1 (96% vs. 74%, P<0.001) and day 7 (91% vs. 63%, P<0.001). Nursing calls were significantly longer than physician calls on both days. A higher adverse event capture rate by physician calls compared to nursing calls was evident on day 1 (3.5% vs. 2.4%, P=0.04) and day 7 (10.6% vs. 6.3%, P=0.004). Physician follow-up calls on day 7 resulted in substantially more patients triaged to the Emergency Department, primary care and oncology clinics (P<0.001).</p><p><strong>Conclusions: </strong>Physician calls were significantly more effective than nurse calls in reaching patients, capturing adverse events, and triaging patients to appropriate care. These data support the value of physician-initiated calls, at least following the most complex procedures.</p>","PeriodicalId":7978,"journal":{"name":"Annals of Gastroenterology","volume":"38 4","pages":"440-445"},"PeriodicalIF":2.2000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12277518/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.20524/aog.2025.0970","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/16 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Endoscopic retrograde cholangiopancreatography (ERCP) is a high-risk endoscopic procedure. We recently found that physician-initiated post-ERCP follow-up calls on day 7 post-ERCP increased adverse event capture. Subsequently, we prospectively evaluated the utility of nurse-initiated follow-up calls, comparing these with physician-initiated calls to assess the impact of transitioning this responsibility to a nurse.
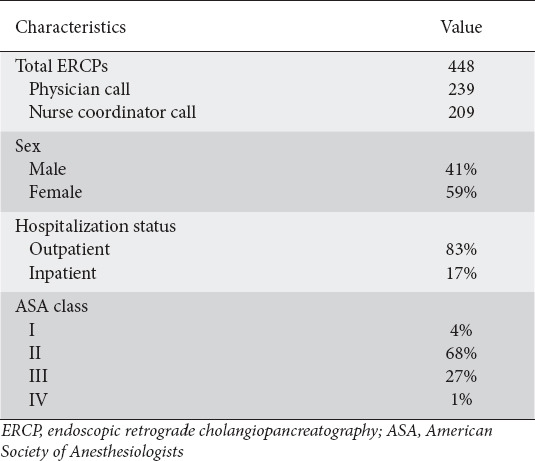
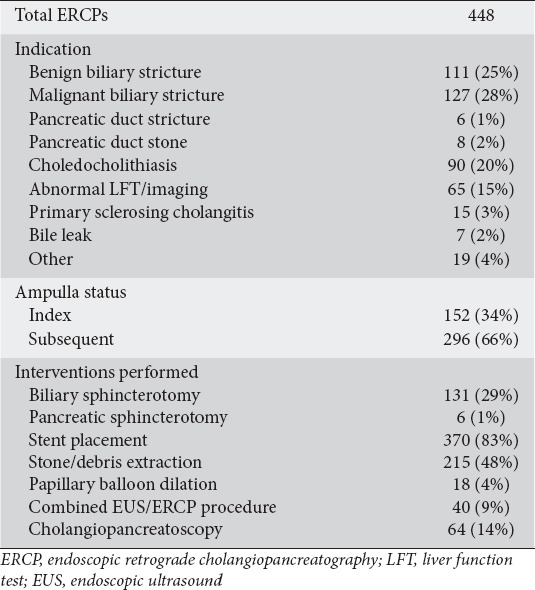
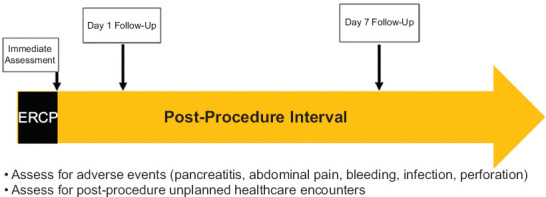
Methods: This prospective study was conducted on consecutive patients undergoing ERCP at our academic tertiary care medical center. Patients received phone calls on days 1 and 7 post-ERCP, from either an endoscopist or a nurse coordinator, using a standardized script to assess delayed complications (pancreatitis, non-pancreatitis abdominal pain, bleeding, infection, perforation), and unplanned health encounters.
Results: A total of 448 ERCP patients (239 physician calls, 209 nursing calls) were included. Physician calls were more successful than nursing calls in reaching patients on both day 1 (96% vs. 74%, P<0.001) and day 7 (91% vs. 63%, P<0.001). Nursing calls were significantly longer than physician calls on both days. A higher adverse event capture rate by physician calls compared to nursing calls was evident on day 1 (3.5% vs. 2.4%, P=0.04) and day 7 (10.6% vs. 6.3%, P=0.004). Physician follow-up calls on day 7 resulted in substantially more patients triaged to the Emergency Department, primary care and oncology clinics (P<0.001).
Conclusions: Physician calls were significantly more effective than nurse calls in reaching patients, capturing adverse events, and triaging patients to appropriate care. These data support the value of physician-initiated calls, at least following the most complex procedures.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


