Association of Difference Between eGFR From Cystatin C and Creatinine and Serum GDF-15 With Adverse Outcomes in Diabetes Mellitus
Abstract
Background
Protein catabolism and chronic inflammation drive sarcopenia and frailty in individuals with diabetes mellitus and chronic kidney disease (CKD). The difference between estimated glomerular filtration rates derived from cystatin C and creatinine (eGFRcys and eGFRcr, respectively), termed eGFRdiff, along with growth differentiation factor-15 (GDF-15) levels, have emerged as markers of metabolic and inflammatory dysregulation. Lower eGFRdiff and elevated GDF-15 levels are associated with sarcopenia, frailty, CKD progression and mortality. However, their interplay and respective impacts on CKD progression and mortality remain unclear.
Methods
A total of 638 Japanese individuals with diabetes mellitus were stratified into tertiles based on eGFRdiff. Serum GDF-15 levels were measured using enzyme-linked immunosorbent assays. The relationships between eGFRdiff and GDF-15 were assessed using Spearman's correlation coefficients. Multivariate ordered logistic regression was used to evaluate the association between eGFRdiff and GDF-15 tertiles, with GDF-15 as the dependent variable and eGFRdiff as the independent variable, adjusting for covariates including age, sex, urinary albumin-to-creatinine ratio (UACR) and eGFRcr or eGFRcys. Cox proportional hazards models with restricted cubic splines were used to examine associations between eGFRdiff and GDF-15 (independent variables) with CKD progression (≥ 30% decline in eGFRcr from baseline) and mortality (dependent variables). These models were adjusted for age, sex, glycated haemoglobin, UACR and eGFRcr.
Results
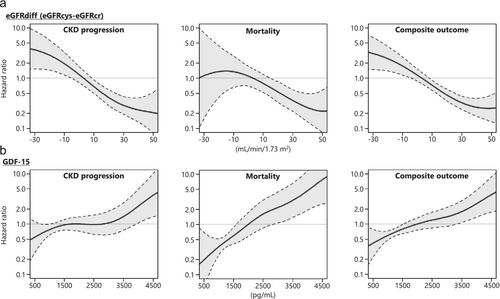
The median age was 65 years (interquartile range: 58–73), and 53.9% of participants were male. Over median follow-up periods of 5.3 years for CKD progression and 5.4 years for mortality, 75 participants (11.8%) experienced CKD progression and 44 (6.9%) died. GDF-15 levels inversely correlated with eGFRdiff (r = −0.35, p < 0.001). Higher eGFRdiff values were associated with lower odds of being in a higher GDF-15 tertile (odds ratio 0.86; 95% confidence interval [CI]: 0.76–0.97; p = 0.01). Both lower eGFRdiff and higher GDF-15 levels were independently associated with adverse outcomes: CKD progression (GDF-15, hazard ratio [HR] 1.36, 95% CI: 1.02–1.81, p < 0.05; eGFRdiff, HR 0.67, 95% CI: 0.58–0.78, p < 0.0001) and mortality (GDF-15, HR 2.35, 95% CI: 1.63–3.41, p < 0.0001; eGFRdiff: 0.80, 95% CI: 0.65–0.99, p < 0.05).
Conclusions
Both eGFRdiff and GDF-15 were independently associated with adverse outcomes in individuals with diabetes mellitus. GDF-15 showed a stronger association with mortality, whereas eGFRdiff was more strongly linked to CKD progression. These findings underscore the potential utility of these markers in risk stratification for diabetes-related complications and may guide individualized interventions in clinical practice.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


