The Oral Health Disparity Among Refugee Children: A Systematic Review
Abstract
Objective
We sought to understand oral health problems among refugee children resettled in developed nations and determine best practices for addressing them.
Methods
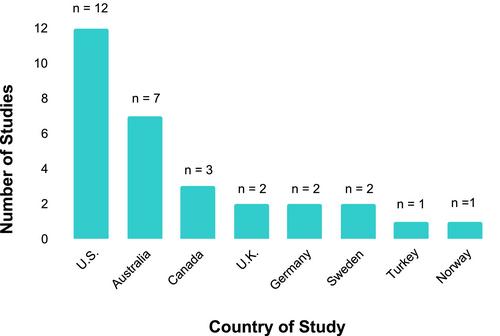
A systematic review was performed and reported in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. A comprehensive search was performed using the PubMed, CINAHL, and Scopus databases from 1980 through 2024 using Medical Subject Heading terms: “children,” “refugee,” and “oral health,” and a separate search in which “oral health” was replaced with “dental caries.” Interventional, qualitative, and epidemiological studies about children resettled in developed nations were included. Critical study appraisal was done using the Critical Appraisal Skills Program (CASP) tool developed at Oxford University. Final data were synthesized in tables and graphs, depicting the study designs, locations, dates of data collection, sample sizes, sample characteristics, and major findings.
Results
Of 30 studies, 25 analyzed oral health in refugee children directly, and six were qualitative studies interviewing parents/caregivers and key informants. Twelve cross-sectional studies included clinical exams, identifying as many as 78% of refugee children with dental caries. Eight studies comparing refugee children to age-and sex-matched children in respective developed countries showed refugee status conferred significantly worse oral health. Two interventional studies demonstrated that parental education improved knowledge but did not improve children's oral health, whereas oral screenings at dedicated refugee health clinics facilitated children receiving referrals and completing treatment. Review data was limited by the lack of standardized or comprehensive measures of oral health.
Conclusions
The refugee pediatric population is at higher risk of oral disease than nonrefugee immigrant and native-born patient populations. Developed nations should address this disparity with community and healthcare partnerships and research, particularly prospective and interventional studies. Otolaryngologists care for the clinical consequences of poor oral health and hygiene and therefore share responsibility in facilitating preventive efforts.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


