Manou Overstijns, Amir El Rahal, Katharina Wolf, Niklas Lützen, Urs Würtemberger, Lucas Becker, Horst Urbach, Daniel Casanova Martinez, Jürgen Beck, Florian Volz
{"title":"Management of chronic subdural hematoma in spontaneous intracranial hypotension.","authors":"Manou Overstijns, Amir El Rahal, Katharina Wolf, Niklas Lützen, Urs Würtemberger, Lucas Becker, Horst Urbach, Daniel Casanova Martinez, Jürgen Beck, Florian Volz","doi":"10.1016/j.bas.2025.104320","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>There is no accepted algorithm for the management of chronic subdural hematoma (cSDH) caused by spinal CSF leaks in spontaneous intracranial hypotension (SIH).</p><p><strong>Research question: </strong>This study analyses characteristics of cSDH in SIH to establish a practicable management algorithm.</p><p><strong>Material and methods: </strong>This retrospective cohort study included all patients with spinal CSF leak closure from April 2018 to April 2024. Demographics, leak type, treatment modalities, as well as cSDH characteristics, prevalence, and risk factors were analyzed.</p><p><strong>Results: </strong>Among 272 SIH patients, 85 (31 %) concomitantly had cSDH, predominantly bilateral (88 %). Hematoma width ranged from 2 to 30 mm. cSDH prevalence was highest in CSF-venous fistulas (43 %), followed by ventral (31 %) and lateral leaks (22 %). Male sex (OR = 4; p < 0.001) and age >70 years (OR = 6; p = 0.008) were significant risk factors. Surgical evacuation was performed in 23 patients, with symptoms attributable to cSDH in 17/23 patients. The biggest cSDH without surgical treatment was 20 mm. No neurological deterioration occurred during diagnostics or treatment of CSF leaks. After leak closure, no cSDH, regardless of initial size or previous treatment, required additional treatment, and no recurrence occurred in the 3-month follow-up.</p><p><strong>Discussion and conclusion: </strong>Primary localization and targeted treatment of the spinal leak is safe in asymptomatic patients and cSDH ≤10 mm (\"leak first\" strategy). Immediate evacuation of the cSDH is mandatory in symptomatic patients (\"subdural first\" strategy). We consider the CSF leak closure as a causal treatment for cSDH resulting in a markedly low, close to zero, recurrence rate. Prospective validation of these findings is needed.</p>","PeriodicalId":72443,"journal":{"name":"Brain & spine","volume":"5 ","pages":"104320"},"PeriodicalIF":2.5000,"publicationDate":"2025-07-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12272930/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Brain & spine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1016/j.bas.2025.104320","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: There is no accepted algorithm for the management of chronic subdural hematoma (cSDH) caused by spinal CSF leaks in spontaneous intracranial hypotension (SIH).
Research question: This study analyses characteristics of cSDH in SIH to establish a practicable management algorithm.
Material and methods: This retrospective cohort study included all patients with spinal CSF leak closure from April 2018 to April 2024. Demographics, leak type, treatment modalities, as well as cSDH characteristics, prevalence, and risk factors were analyzed.
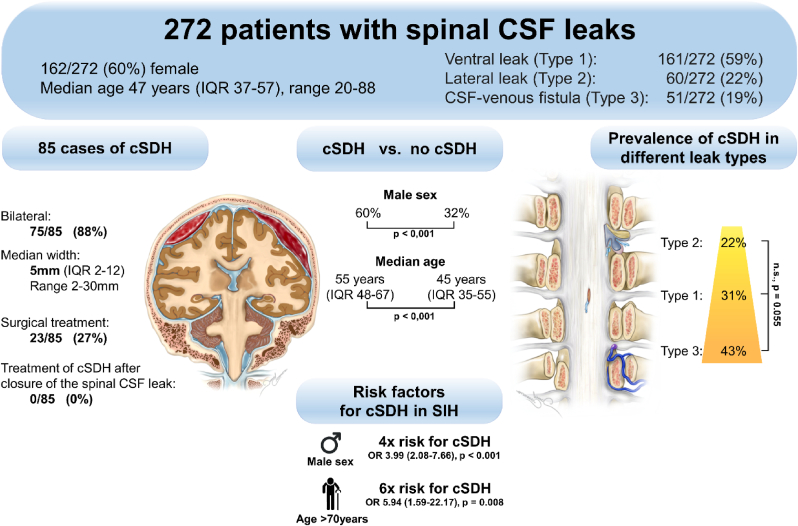
Results: Among 272 SIH patients, 85 (31 %) concomitantly had cSDH, predominantly bilateral (88 %). Hematoma width ranged from 2 to 30 mm. cSDH prevalence was highest in CSF-venous fistulas (43 %), followed by ventral (31 %) and lateral leaks (22 %). Male sex (OR = 4; p < 0.001) and age >70 years (OR = 6; p = 0.008) were significant risk factors. Surgical evacuation was performed in 23 patients, with symptoms attributable to cSDH in 17/23 patients. The biggest cSDH without surgical treatment was 20 mm. No neurological deterioration occurred during diagnostics or treatment of CSF leaks. After leak closure, no cSDH, regardless of initial size or previous treatment, required additional treatment, and no recurrence occurred in the 3-month follow-up.
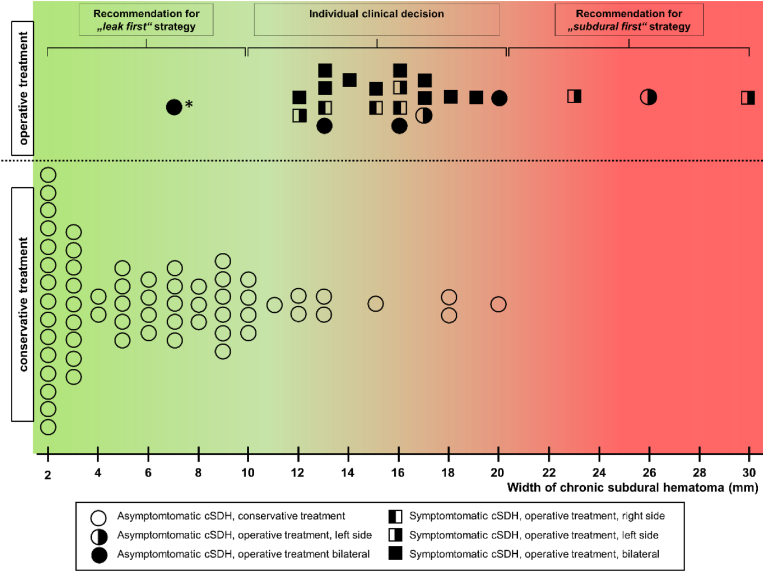
Discussion and conclusion: Primary localization and targeted treatment of the spinal leak is safe in asymptomatic patients and cSDH ≤10 mm ("leak first" strategy). Immediate evacuation of the cSDH is mandatory in symptomatic patients ("subdural first" strategy). We consider the CSF leak closure as a causal treatment for cSDH resulting in a markedly low, close to zero, recurrence rate. Prospective validation of these findings is needed.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


