Kevin Y Wang, Alexander R Farid, Simon Comtesse, Arvind G von Keudell
{"title":"Segmentation and finite element analysis in orthopaedic trauma.","authors":"Kevin Y Wang, Alexander R Farid, Simon Comtesse, Arvind G von Keudell","doi":"10.1186/s41205-025-00284-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Finite Element Analysis (FEA) has evolved into a crucial tool in orthopaedic trauma research and clinical practice. This review explores the broad applications of FEA in orthopedic surgery.</p><p><strong>Main body: </strong>FEA involves several steps, including geometry representation, segmentation, 3D rendering, meshing, material property assignment, defining boundary conditions, and specifying contact conditions. The process utilizes patient-specific volumetric data-computed tomography (CT) scan, for example-and aims for a balance between computational efficiency and accuracy. FEA provides valuable outcome measures such as stress distribution, strain quantification, fracture gap motion, failure prediction, and implant stability. These measures aid in evaluating fracture fixation techniques, implant design, and the impact of different fixation strategies. FEA has found applications in femur and proximal humerus fracture fixation, distal femur fracture planning, tibial plateau fractures, and post-traumatic osteoarthritis. It plays a pivotal role in predicting fracture risk, assessing construct stability, and informing surgical decision-making. Additionally, FEA facilitates the development of custom surgical planning and personalized implants. To enhance accuracy, FEA is combined with cadaveric biomechanical analysis, providing a reference-standard representation of in vivo kinematics. Future research should focus on refining FEA models through increased validation using cadaveric models and clinical data.</p><p><strong>Conclusion: </strong>FEA has revolutionized orthopaedic trauma research by offering insights into biomechanics, fracture fixation, and implant design. Integration with cadaveric biomechanical analysis enhances accuracy. Further validation efforts and integration into regular clinical practice are essential for realizing FEA's full potential in individualized patient care. The combination of FEA and cadaveric analysis contributes to a comprehensive understanding of in vivo kinematics, ultimately improving patient outcomes.</p>","PeriodicalId":72036,"journal":{"name":"3D printing in medicine","volume":"11 1","pages":"39"},"PeriodicalIF":3.1000,"publicationDate":"2025-07-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12278576/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"3D printing in medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s41205-025-00284-9","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Finite Element Analysis (FEA) has evolved into a crucial tool in orthopaedic trauma research and clinical practice. This review explores the broad applications of FEA in orthopedic surgery.
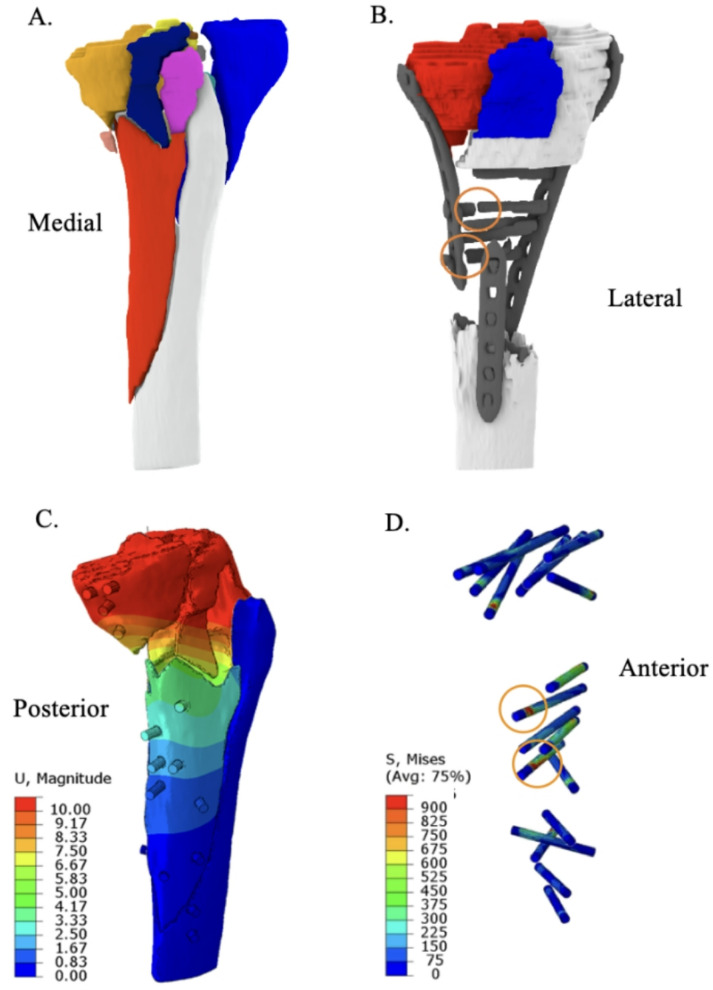
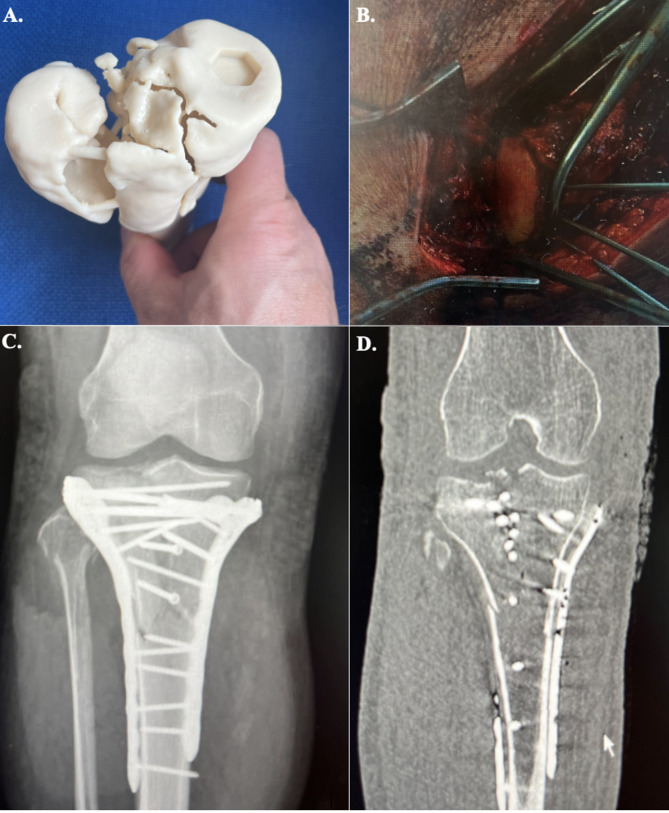
Main body: FEA involves several steps, including geometry representation, segmentation, 3D rendering, meshing, material property assignment, defining boundary conditions, and specifying contact conditions. The process utilizes patient-specific volumetric data-computed tomography (CT) scan, for example-and aims for a balance between computational efficiency and accuracy. FEA provides valuable outcome measures such as stress distribution, strain quantification, fracture gap motion, failure prediction, and implant stability. These measures aid in evaluating fracture fixation techniques, implant design, and the impact of different fixation strategies. FEA has found applications in femur and proximal humerus fracture fixation, distal femur fracture planning, tibial plateau fractures, and post-traumatic osteoarthritis. It plays a pivotal role in predicting fracture risk, assessing construct stability, and informing surgical decision-making. Additionally, FEA facilitates the development of custom surgical planning and personalized implants. To enhance accuracy, FEA is combined with cadaveric biomechanical analysis, providing a reference-standard representation of in vivo kinematics. Future research should focus on refining FEA models through increased validation using cadaveric models and clinical data.
Conclusion: FEA has revolutionized orthopaedic trauma research by offering insights into biomechanics, fracture fixation, and implant design. Integration with cadaveric biomechanical analysis enhances accuracy. Further validation efforts and integration into regular clinical practice are essential for realizing FEA's full potential in individualized patient care. The combination of FEA and cadaveric analysis contributes to a comprehensive understanding of in vivo kinematics, ultimately improving patient outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


