Contribution of intravenous medication diluent fluid composition on the development of dyschloremia in intensive care unit patients: A retrospective chart review.
{"title":"Contribution of intravenous medication diluent fluid composition on the development of dyschloremia in intensive care unit patients: A retrospective chart review.","authors":"Mahsa Movahedan, Glen Brown","doi":"10.1177/20503121251356069","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Intravenous solutions such as dextrose 5% in water and 0.9% sodium chloride (normal saline) differ in electrolyte composition from human plasma and may contribute to serum chloride derangements (dyschloremia). This retrospective study aimed to explore the relationship between fluid composition, particularly medication diluents, and dyschloremia development in the intensive care unit.</p><p><strong>Methods: </strong>This was a retrospective chart review of adult intensive care unit patients with normal serum chloride on admission who developed dyschloremia after 48 h of intensive care unit admission. Data were collected on fluid types and volumes administered in the intensive care unit in the 7 days prior to dyschloremia onset. Descriptive statistics and chi-square tests were used to compare characteristics between patients who developed hyperchloremia and hypochloremia.</p><p><strong>Results: </strong>Of 884 screened patients, 85 developed dyschloremia after 48 h (41 hypochloremia, 44 hyperchloremia). There was no significant association between the proportion of normal saline or dextrose 5% in water-containing fluids and the type of dyschloremia. However, dexmedetomidine, typically diluted in normal saline, was associated with hyperchloremia.</p><p><strong>Conclusion: </strong>While total fluid composition was not associated with dyschloremia type, high-volume use of specific diluent-medication combinations may contribute. Strategies to minimize diluent volume could help reduce dyschloremia risk.</p>","PeriodicalId":21398,"journal":{"name":"SAGE Open Medicine","volume":"13 ","pages":"20503121251356069"},"PeriodicalIF":2.1000,"publicationDate":"2025-07-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12276513/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"SAGE Open Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20503121251356069","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Intravenous solutions such as dextrose 5% in water and 0.9% sodium chloride (normal saline) differ in electrolyte composition from human plasma and may contribute to serum chloride derangements (dyschloremia). This retrospective study aimed to explore the relationship between fluid composition, particularly medication diluents, and dyschloremia development in the intensive care unit.
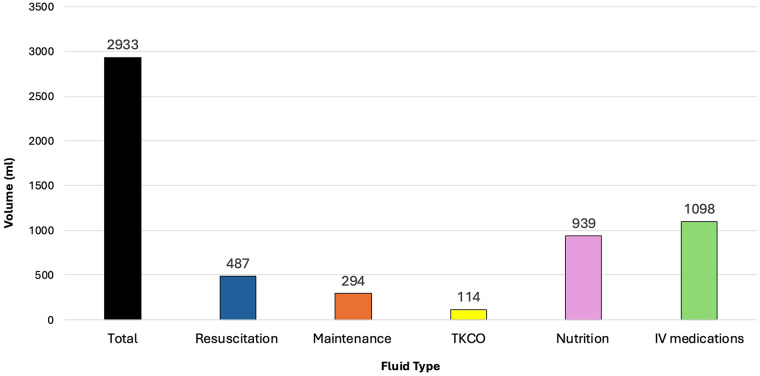
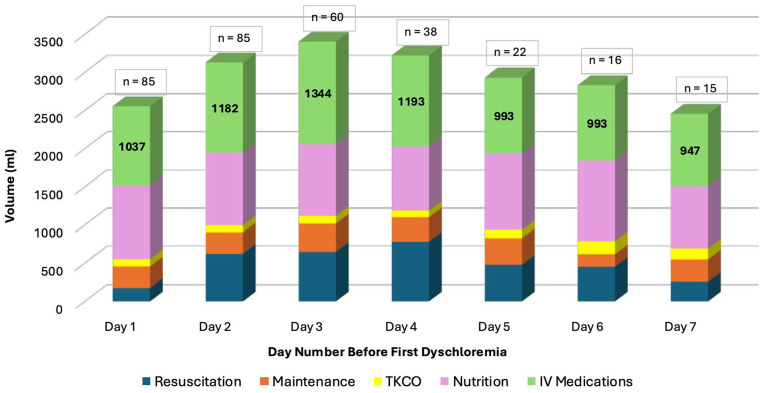
Methods: This was a retrospective chart review of adult intensive care unit patients with normal serum chloride on admission who developed dyschloremia after 48 h of intensive care unit admission. Data were collected on fluid types and volumes administered in the intensive care unit in the 7 days prior to dyschloremia onset. Descriptive statistics and chi-square tests were used to compare characteristics between patients who developed hyperchloremia and hypochloremia.
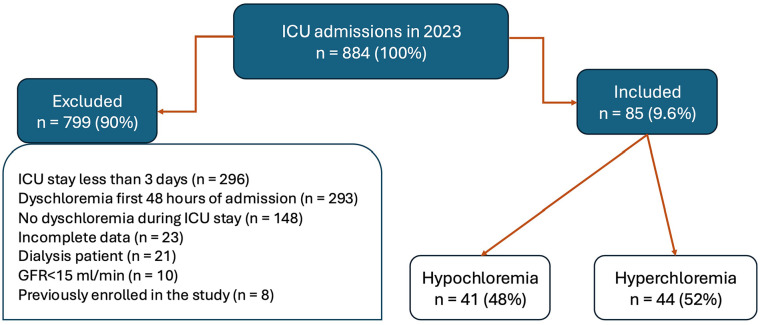
Results: Of 884 screened patients, 85 developed dyschloremia after 48 h (41 hypochloremia, 44 hyperchloremia). There was no significant association between the proportion of normal saline or dextrose 5% in water-containing fluids and the type of dyschloremia. However, dexmedetomidine, typically diluted in normal saline, was associated with hyperchloremia.
Conclusion: While total fluid composition was not associated with dyschloremia type, high-volume use of specific diluent-medication combinations may contribute. Strategies to minimize diluent volume could help reduce dyschloremia risk.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


