{"title":"The Learning Curve for Transoral Endoscopic Thyroidectomy Without Neuromonitoring: Analysis of First 103 Cases From India.","authors":"Sanjay Kumar Yadav, Goonj Johri, Saket Shekhar, Pawan Agarwal, Dhananjaya Sharma","doi":"10.1002/oto2.70142","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Transoral endoscopic thyroidectomy via the vestibular approach (TOETVA) offers a scarless alternative to conventional thyroidectomy. Most studies incorporate intraoperative neuromonitoring (IONM), which may be unavailable in resource-limited settings. We evaluated the learning curve, feasibility, and safety of TOETVA without IONM.</p><p><strong>Study design: </strong>Retrospective.</p><p><strong>Setting: </strong>A retrospective analysis of 103 patients undergoing hemithyroidectomy by TOETVA between February 2020 and January 2025 was conducted at a tertiary care center in central India.</p><p><strong>Method: </strong>Learning curve assessment was performed using Cumulative Sum (CUSUM) analysis, and outcomes were compared between phase 1 (cases 1-50) and phase 2 (Cases 51-103). Statistical analyses included independent <i>t</i> tests for continuous variables and chi-square tests for categorical variables (<i>P</i> < .05).</p><p><strong>Results: </strong>Mean operative time significantly decreased from 185 ± 24 minutes in phase 1 to 105 ± 12.95 minutes in phase 2 (<i>P</i> < .001), with proficiency achieved after 50 cases. Nodule size was larger in phase 2 (4.5 ± 2.3 cm vs 3.0 ± 1.0 cm, <i>P</i> = .003). The conversion rate was 4.9%, with no permanent recurrent laryngeal nerve palsy. Hoarseness of voice and seroma rates remained unchanged (<i>P</i> = 1.00), whereas hospital stay significantly decreased (<i>P</i> < .001).</p><p><strong>Conclusion: </strong>TOETVA without IONM is feasible and safe, demonstrating a well-defined learning curve with low complication rates. These findings support its adoption in low-resource settings.</p>","PeriodicalId":19697,"journal":{"name":"OTO Open","volume":"9 3","pages":"e70142"},"PeriodicalIF":1.8000,"publicationDate":"2025-07-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12271831/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"OTO Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1002/oto2.70142","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"OTORHINOLARYNGOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Transoral endoscopic thyroidectomy via the vestibular approach (TOETVA) offers a scarless alternative to conventional thyroidectomy. Most studies incorporate intraoperative neuromonitoring (IONM), which may be unavailable in resource-limited settings. We evaluated the learning curve, feasibility, and safety of TOETVA without IONM.
Study design: Retrospective.
Setting: A retrospective analysis of 103 patients undergoing hemithyroidectomy by TOETVA between February 2020 and January 2025 was conducted at a tertiary care center in central India.
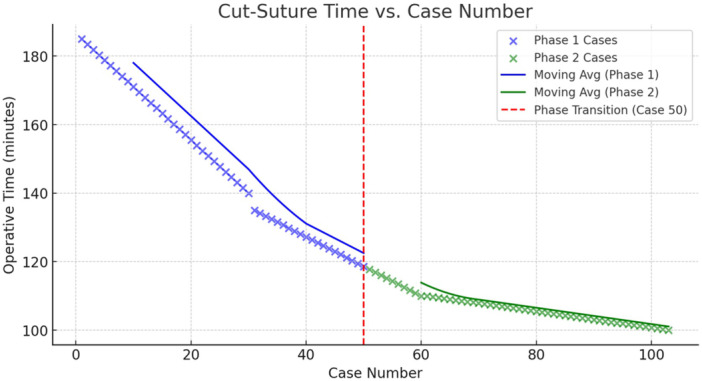
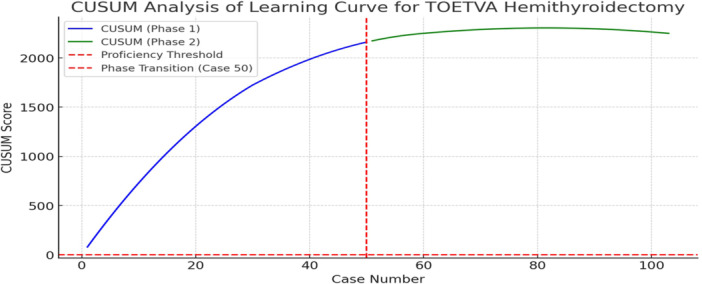
Method: Learning curve assessment was performed using Cumulative Sum (CUSUM) analysis, and outcomes were compared between phase 1 (cases 1-50) and phase 2 (Cases 51-103). Statistical analyses included independent t tests for continuous variables and chi-square tests for categorical variables (P < .05).
Results: Mean operative time significantly decreased from 185 ± 24 minutes in phase 1 to 105 ± 12.95 minutes in phase 2 (P < .001), with proficiency achieved after 50 cases. Nodule size was larger in phase 2 (4.5 ± 2.3 cm vs 3.0 ± 1.0 cm, P = .003). The conversion rate was 4.9%, with no permanent recurrent laryngeal nerve palsy. Hoarseness of voice and seroma rates remained unchanged (P = 1.00), whereas hospital stay significantly decreased (P < .001).
Conclusion: TOETVA without IONM is feasible and safe, demonstrating a well-defined learning curve with low complication rates. These findings support its adoption in low-resource settings.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


