Ahmed Mohamed Ibrahim, Mohammed Said ElSharkawy, Reda Khalil Abdelrahman, Abdallah Elabd Hassan, Mohammed Gaber Ibrahim Saad, Ismail Ahmed Elzoughari, Abdelkarem Hussini Ismail Alsayed, Asmaa Abdelbadie, Rehab Abd El Fattah Helal
{"title":"Deep Neuromuscular Block with Low Pressure Pneumoperitoneum in Laparoscopic Abdominal Surgeries: A Randomized Controlled Trial.","authors":"Ahmed Mohamed Ibrahim, Mohammed Said ElSharkawy, Reda Khalil Abdelrahman, Abdallah Elabd Hassan, Mohammed Gaber Ibrahim Saad, Ismail Ahmed Elzoughari, Abdelkarem Hussini Ismail Alsayed, Asmaa Abdelbadie, Rehab Abd El Fattah Helal","doi":"10.5812/aapm-150995","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Postoperative pain management remains a challenge in laparoscopic abdominal surgeries.</p><p><strong>Objectives: </strong>The purpose of this research was to determine the effects of deep neuromuscular blockade (NMB) in conjunction with low-pressure pneumoperitoneum )PP) on postoperative pain, surgical parameters, and recovery outcomes.</p><p><strong>Methods: </strong>This randomized controlled double-blind study included 44 participants undergoing laparoscopic abdominal surgery. Patients were randomized equally into two groups (22 each): Group D received deep NMB, while group M received moderate NMB using cis-atracurium, through the utilization of computer-generated random numbers enclosed within sealed, opaque envelopes, following a parallel approach. Regarding deep NMB, following an initial dose of 0.15 mg/kg, a continuous infusion of 0.06 - 0.12 mg/kg/hr was administered to maintain a post-tetanic count between 1 and 2, with low PP pressure of 10 - 12 mmHg. Conversely, for moderate NMB, after the same initial dose of 0.15 mg/kg, the continuous infusion commenced upon the train-of-four count returning to 2, with the rate adjusted to sustain a count between 1 and 3, and standard PP pressure of 15 mmHg. The primary outcome was postoperative pain intensity as measured by Numerical Rating Scale (NRS) scores in the post-anesthesia care unit (PACU). The secondary outcomes included postoperative pain intensity measured by NRS scores from 2 hours to 48 hours post-surgery, time to first analgesic administration, cumulative opioid consumption within the initial 48-hour postoperative period, and patient-reported satisfaction with postoperative pain management. Statistical analysis using SPSS v26 included tests for normality (Shapiro-Wilks), with parametric data analyzed by <i>t</i>-test, non-parametric data by Mann-Whitney, and qualitative data by chi-square/Fisher's test.</p><p><strong>Results: </strong>Group D experienced a considerably longer time until the first analgesic rescue compared to group M (9.82 ± 1.5 hours vs. 7.23 ± 1.19 hours, P < 0.001). Morphine consumption in the first 24 hours was lower in Group D (10.77 ± 1.51 mg vs. 13.09 ± 1.74 mg, P < 0.001). At 6, 8, and 12 hours postoperatively, group D exhibited significantly lower pain scores (P < 0.05). Surgical duration, surgical field quality, complication rates, and patient satisfaction were comparable between groups.</p><p><strong>Conclusions: </strong>Deep NMB combined with low-pressure PP provided superior postoperative analgesia without compromising surgical field quality or increasing complications in laparoscopic abdominal surgeries.</p>","PeriodicalId":7841,"journal":{"name":"Anesthesiology and Pain Medicine","volume":"14 5","pages":"e150995"},"PeriodicalIF":0.0000,"publicationDate":"2024-10-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12275633/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Anesthesiology and Pain Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5812/aapm-150995","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Postoperative pain management remains a challenge in laparoscopic abdominal surgeries.
Objectives: The purpose of this research was to determine the effects of deep neuromuscular blockade (NMB) in conjunction with low-pressure pneumoperitoneum )PP) on postoperative pain, surgical parameters, and recovery outcomes.
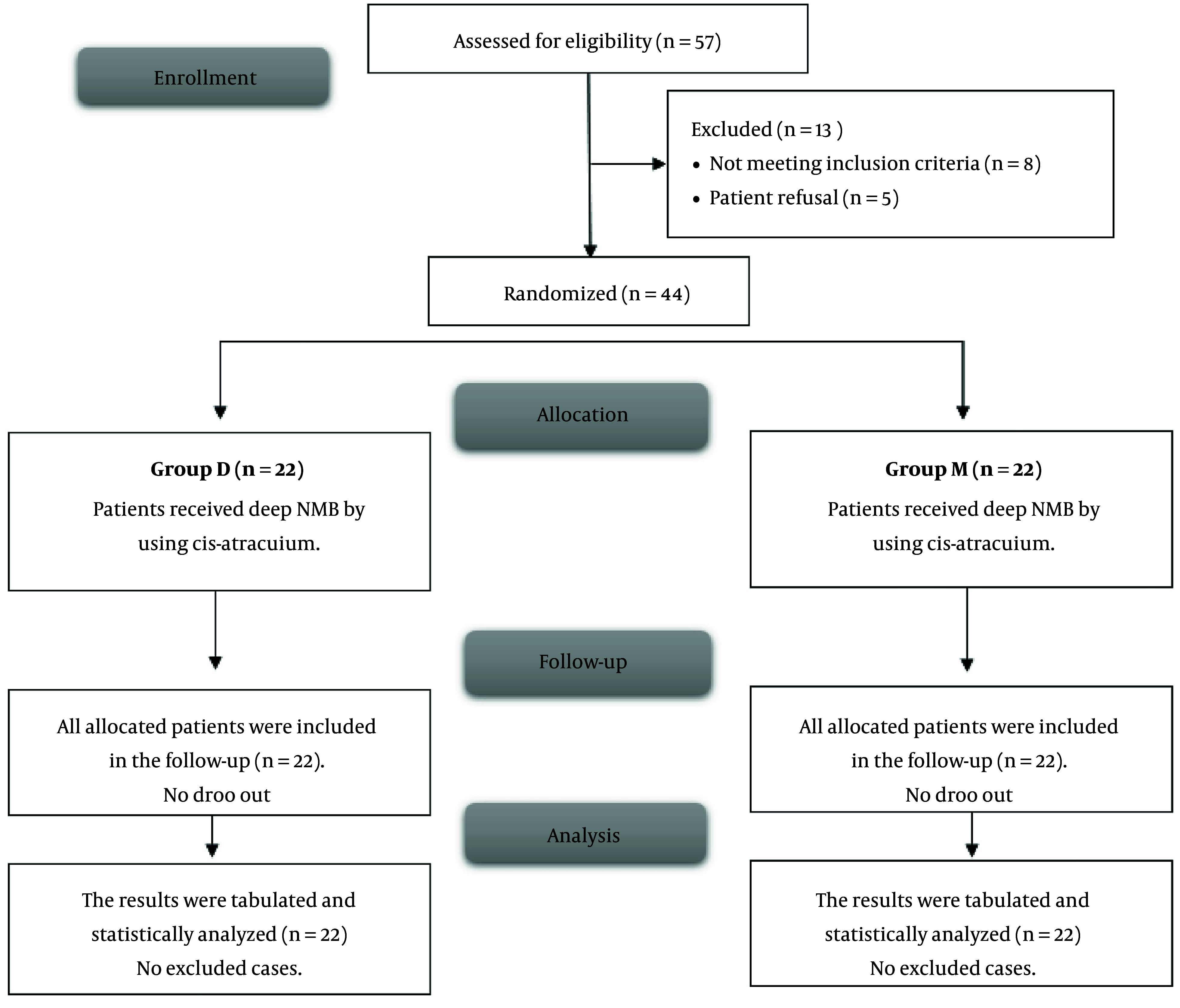
Methods: This randomized controlled double-blind study included 44 participants undergoing laparoscopic abdominal surgery. Patients were randomized equally into two groups (22 each): Group D received deep NMB, while group M received moderate NMB using cis-atracurium, through the utilization of computer-generated random numbers enclosed within sealed, opaque envelopes, following a parallel approach. Regarding deep NMB, following an initial dose of 0.15 mg/kg, a continuous infusion of 0.06 - 0.12 mg/kg/hr was administered to maintain a post-tetanic count between 1 and 2, with low PP pressure of 10 - 12 mmHg. Conversely, for moderate NMB, after the same initial dose of 0.15 mg/kg, the continuous infusion commenced upon the train-of-four count returning to 2, with the rate adjusted to sustain a count between 1 and 3, and standard PP pressure of 15 mmHg. The primary outcome was postoperative pain intensity as measured by Numerical Rating Scale (NRS) scores in the post-anesthesia care unit (PACU). The secondary outcomes included postoperative pain intensity measured by NRS scores from 2 hours to 48 hours post-surgery, time to first analgesic administration, cumulative opioid consumption within the initial 48-hour postoperative period, and patient-reported satisfaction with postoperative pain management. Statistical analysis using SPSS v26 included tests for normality (Shapiro-Wilks), with parametric data analyzed by t-test, non-parametric data by Mann-Whitney, and qualitative data by chi-square/Fisher's test.
Results: Group D experienced a considerably longer time until the first analgesic rescue compared to group M (9.82 ± 1.5 hours vs. 7.23 ± 1.19 hours, P < 0.001). Morphine consumption in the first 24 hours was lower in Group D (10.77 ± 1.51 mg vs. 13.09 ± 1.74 mg, P < 0.001). At 6, 8, and 12 hours postoperatively, group D exhibited significantly lower pain scores (P < 0.05). Surgical duration, surgical field quality, complication rates, and patient satisfaction were comparable between groups.
Conclusions: Deep NMB combined with low-pressure PP provided superior postoperative analgesia without compromising surgical field quality or increasing complications in laparoscopic abdominal surgeries.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


