Adriana Baez, Gabriele Tonni, Chryso P Katsoufis, Amanda Alladin, Ugo Maria Pierucci, Yair J Blumenfeld, Rodrigo Ruano
{"title":"Serial Amnioinfusion Therapy for Treatment of Congenital Bilateral Renal Agenesis-A Systematic Review.","authors":"Adriana Baez, Gabriele Tonni, Chryso P Katsoufis, Amanda Alladin, Ugo Maria Pierucci, Yair J Blumenfeld, Rodrigo Ruano","doi":"10.1002/pd.6850","DOIUrl":null,"url":null,"abstract":"<p><p>Serial amnioinfusion therapy (SAT) has emerged as a potential mitigatory intervention to adverse perinatal outcomes associated with congenital bilateral renal agenesis (BRA). However, its efficacy, safety, and ethical implications warrant thorough evaluation. This systematic review, developed according to PRISMA guidelines, analyzes the published data on outcomes of SAT for BRA and explores its implications. Inclusion criteria were a diagnosis of bilateral renal agenesis, therapeutic use of amnioinfusion, amnioinfusion procedure, and individual maternal and fetal outcome reports. A total of 192 published studies were identified. Among these, 11 full texts were included (N = 40). Only cases resulting in live birth and with reported maternal and neonatal outcomes were analyzed. The average number of amnioinfusions per mother was 9 (n = 23; range 1-26 infusions). Median gestational age at delivery was 33.4 weeks (n = 40; range 23.7-36.8 weeks). APGAR scores (n = 14) at 1 and 5 min were 4 and 6, respectively. Almost half of newborns died within 33 days of life (n = 19) and 7 (17.5%) survived at the time of original publication. Overall neonatal mortality was 82.5% (33 of 40). These findings suggest that SAT for BRA improves the chances of neonatal survival in the first few days to weeks of life but not consistently beyond that time. Additional advances in neonatal care are needed to improve long-term outcomes in peripartum survivors.</p>","PeriodicalId":20387,"journal":{"name":"Prenatal Diagnosis","volume":" ","pages":"1182-1191"},"PeriodicalIF":2.7000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12322254/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Prenatal Diagnosis","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/pd.6850","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/18 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"GENETICS & HEREDITY","Score":null,"Total":0}
引用次数: 0
Abstract
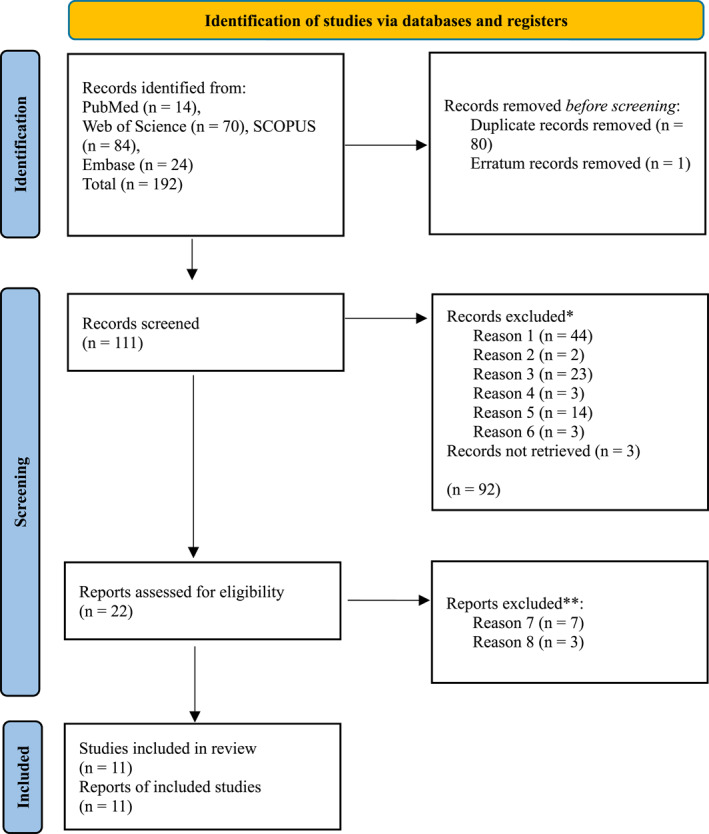
Serial amnioinfusion therapy (SAT) has emerged as a potential mitigatory intervention to adverse perinatal outcomes associated with congenital bilateral renal agenesis (BRA). However, its efficacy, safety, and ethical implications warrant thorough evaluation. This systematic review, developed according to PRISMA guidelines, analyzes the published data on outcomes of SAT for BRA and explores its implications. Inclusion criteria were a diagnosis of bilateral renal agenesis, therapeutic use of amnioinfusion, amnioinfusion procedure, and individual maternal and fetal outcome reports. A total of 192 published studies were identified. Among these, 11 full texts were included (N = 40). Only cases resulting in live birth and with reported maternal and neonatal outcomes were analyzed. The average number of amnioinfusions per mother was 9 (n = 23; range 1-26 infusions). Median gestational age at delivery was 33.4 weeks (n = 40; range 23.7-36.8 weeks). APGAR scores (n = 14) at 1 and 5 min were 4 and 6, respectively. Almost half of newborns died within 33 days of life (n = 19) and 7 (17.5%) survived at the time of original publication. Overall neonatal mortality was 82.5% (33 of 40). These findings suggest that SAT for BRA improves the chances of neonatal survival in the first few days to weeks of life but not consistently beyond that time. Additional advances in neonatal care are needed to improve long-term outcomes in peripartum survivors.
期刊介绍:
Prenatal Diagnosis welcomes submissions in all aspects of prenatal diagnosis with a particular focus on areas in which molecular biology and genetics interface with prenatal care and therapy, encompassing: all aspects of fetal imaging, including sonography and magnetic resonance imaging; prenatal cytogenetics, including molecular studies and array CGH; prenatal screening studies; fetal cells and cell-free nucleic acids in maternal blood and other fluids; preimplantation genetic diagnosis (PGD); prenatal diagnosis of single gene disorders, including metabolic disorders; fetal therapy; fetal and placental development and pathology; development and evaluation of laboratory services for prenatal diagnosis; psychosocial, legal, ethical and economic aspects of prenatal diagnosis; prenatal genetic counseling

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


