The incidence of vascular adverse events and usefulness of novel risk assessment tool in Japanese patients with chronic myeloid leukemia treated with tyrosine kinase inhibitors.
{"title":"The incidence of vascular adverse events and usefulness of novel risk assessment tool in Japanese patients with chronic myeloid leukemia treated with tyrosine kinase inhibitors.","authors":"Naoki Watanabe, Tomoiku Takaku, Noriyoshi Iriyama, Eisaku Iwanaga, Yuta Kimura, Maho Ishikawa, Hitomi Nakayama, Eriko Sato, Takayuki Tabayashi, Toru Mitsumori, Tomonori Nakazato, Michihide Tokuhira, Hiroyuki Fujita, Miki Ando, Katsuhiro Miura, Tatsuya Kawaguchi","doi":"10.1186/s40959-025-00366-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Tyrosine kinase inhibitor (TKI) therapy improves the overall survival of patients with chronic myeloid leukemia (CML). However, the risk of vascular adverse events (VAEs) in these patients is reported to be higher than that in healthy individuals, because of both CML itself and the effects of TKIs. Appropriate and effective VAE risk assessment tools for TKI treatment have long been anticipated.</p><p><strong>Methods: </strong>Here, we investigated the usefulness of a newly developed VAE risk assessment tool, the Hisayama score, and presented data on the clinical characteristics of VAEs in Japanese patients with CML based on an analysis of a real-world, large-cohort database.</p><p><strong>Results: </strong>Patients with CML who developed VAEs were evaluated using three VAE risk assessment tools. Forty-four VAEs were reported in 41 out of 626 patients with CML, with three patients developing multiple VAEs during the observation period. There were 16 cases of cerebral infarction, 19 of ischemic heart disease, and nine of peripheral artery occlusive disease, with rates per 1,000 person-years of 3.23, 3.84, and 2.02, respectively. The Framingham and Hisayama scores stratified high-risk patients with VAEs more effectively than the SCORE chart. Smoking and hypertension are prominent risk factors for VAEs.</p><p><strong>Conclusions: </strong>Our results clearly demonstrate that the Hisayama score can be used to evaluate VAE risk in high-risk patients. Selecting appropriate TKIs based on each patient risk, smoking cessation, and blood pressure control may contribute to selecting appropriate TKIs and managing VAE risk.</p>","PeriodicalId":9804,"journal":{"name":"Cardio-oncology","volume":"11 1","pages":"68"},"PeriodicalIF":3.2000,"publicationDate":"2025-07-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12275440/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardio-oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40959-025-00366-x","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Tyrosine kinase inhibitor (TKI) therapy improves the overall survival of patients with chronic myeloid leukemia (CML). However, the risk of vascular adverse events (VAEs) in these patients is reported to be higher than that in healthy individuals, because of both CML itself and the effects of TKIs. Appropriate and effective VAE risk assessment tools for TKI treatment have long been anticipated.
Methods: Here, we investigated the usefulness of a newly developed VAE risk assessment tool, the Hisayama score, and presented data on the clinical characteristics of VAEs in Japanese patients with CML based on an analysis of a real-world, large-cohort database.
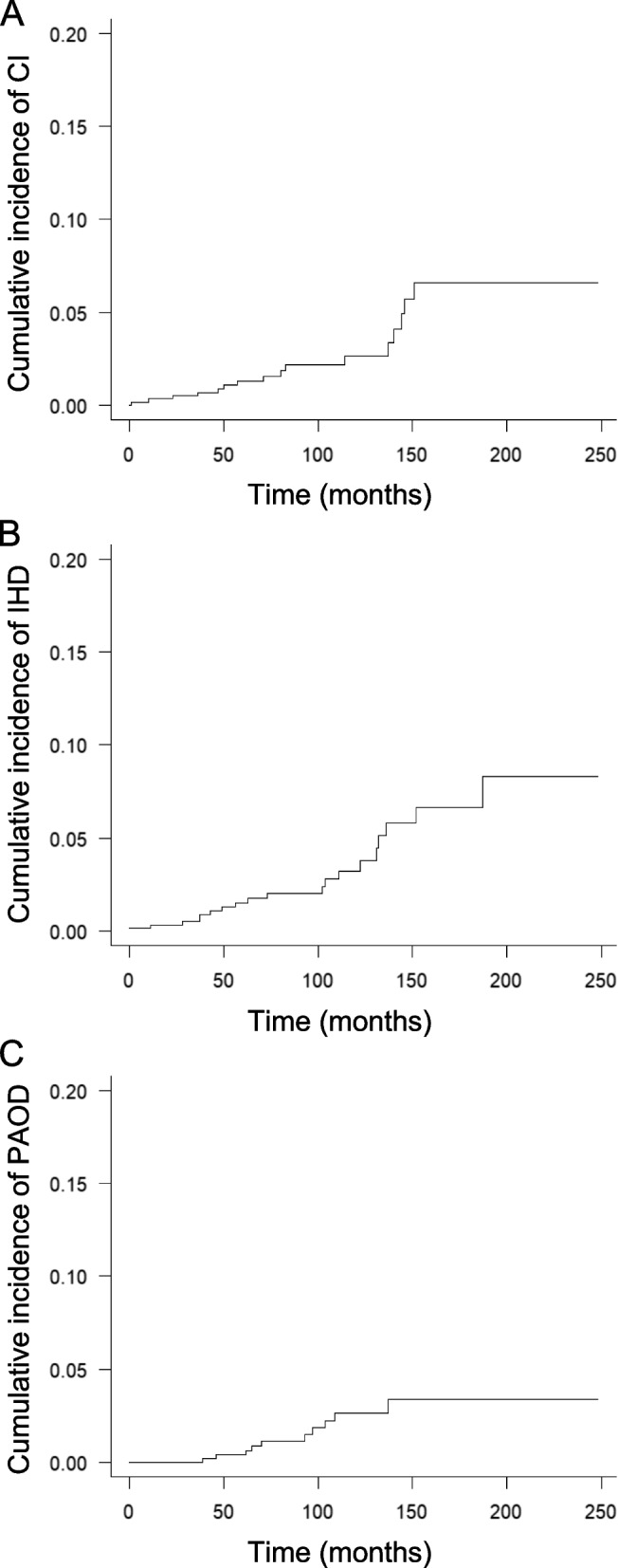
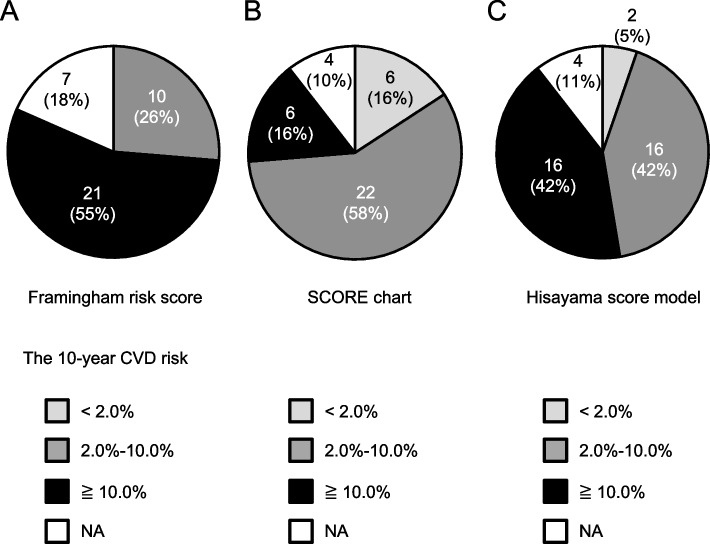
Results: Patients with CML who developed VAEs were evaluated using three VAE risk assessment tools. Forty-four VAEs were reported in 41 out of 626 patients with CML, with three patients developing multiple VAEs during the observation period. There were 16 cases of cerebral infarction, 19 of ischemic heart disease, and nine of peripheral artery occlusive disease, with rates per 1,000 person-years of 3.23, 3.84, and 2.02, respectively. The Framingham and Hisayama scores stratified high-risk patients with VAEs more effectively than the SCORE chart. Smoking and hypertension are prominent risk factors for VAEs.
Conclusions: Our results clearly demonstrate that the Hisayama score can be used to evaluate VAE risk in high-risk patients. Selecting appropriate TKIs based on each patient risk, smoking cessation, and blood pressure control may contribute to selecting appropriate TKIs and managing VAE risk.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


