Sheyda Mesgarzadeh BS , Rosemond S. Amamoo MD, MPH , Geethika Ameneni BS , Amanda H. Gong BS , Oluwayemisi O. Ayoade MD, MPH , Delaney B. Stratton PhD, DNP , Emile Latour PhD, MPH , Wesley Yu MD , Clara Curiel-Lewandrowski MD , Ivo Abraham PhD , Mohammad Fazel MD, PharmD
{"title":"Validation of risk prediction models for sentinel lymph node metastasis in melanoma in a high UV index region","authors":"Sheyda Mesgarzadeh BS , Rosemond S. Amamoo MD, MPH , Geethika Ameneni BS , Amanda H. Gong BS , Oluwayemisi O. Ayoade MD, MPH , Delaney B. Stratton PhD, DNP , Emile Latour PhD, MPH , Wesley Yu MD , Clara Curiel-Lewandrowski MD , Ivo Abraham PhD , Mohammad Fazel MD, PharmD","doi":"10.1016/j.jdin.2025.04.012","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><div>Risk prediction models may refine individualized selection for sentinel lymph node biopsy (SLNB) in melanoma.</div></div><div><h3>Objective</h3><div>To evaluate the statistical accuracy and clinical utility of nomograms by the Melanoma Institute of Australia (MIA), Memorial Sloan Kettering Cancer Center (MSKCC), and University of Colorado in a Southern Arizona population.</div></div><div><h3>Methods</h3><div>In this prognostic validation, statistical accuracy was assessed through discrimination, measured with receiver operating characteristic curves and calibration plots. Clinical utility was evaluated via decision curve analysis to determine the net benefit and number of net avoidable interventions achieved with nomogram use.</div></div><div><h3>Results</h3><div>Among 712 melanoma cases included, model discrimination was highest for the MIA nomogram (C-statistic = 0.753; 95% confidence interval = 0.694-0.812), followed by MSKCC (0.729[0.671-0.787]), and University of Colorado (0.601[0.405-0.793]). The MIA and MSKCC nomograms were well-calibrated across clinically relevant risk thresholds. All nomograms achieved a net benefit and net reduction in avoidable SLNBs for risk thresholds ≥5%. There was minimal to no reduction in unnecessary interventions at age extremes (<50 and ≥ 80 years old) for specific risk strata and nomograms.</div></div><div><h3>Limitations</h3><div>This a 5-year retrospective study.</div></div><div><h3>Conclusions</h3><div>These nomograms can be used to support SLNB decision-making in this population but necessitate caution in patients at age extremes when used to reduce avoidable interventions.</div></div>","PeriodicalId":34410,"journal":{"name":"JAAD International","volume":"21 ","pages":"Pages 61-69"},"PeriodicalIF":5.2000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JAAD International","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2666328725000495","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Risk prediction models may refine individualized selection for sentinel lymph node biopsy (SLNB) in melanoma.
Objective
To evaluate the statistical accuracy and clinical utility of nomograms by the Melanoma Institute of Australia (MIA), Memorial Sloan Kettering Cancer Center (MSKCC), and University of Colorado in a Southern Arizona population.
Methods
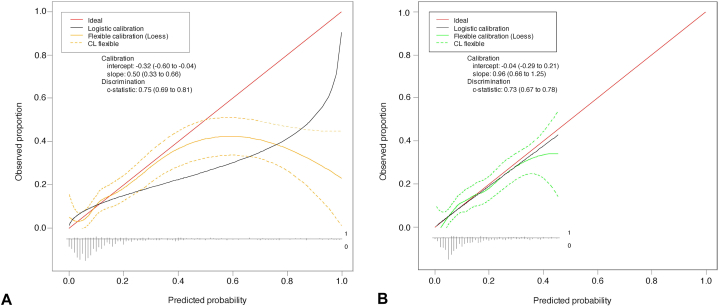
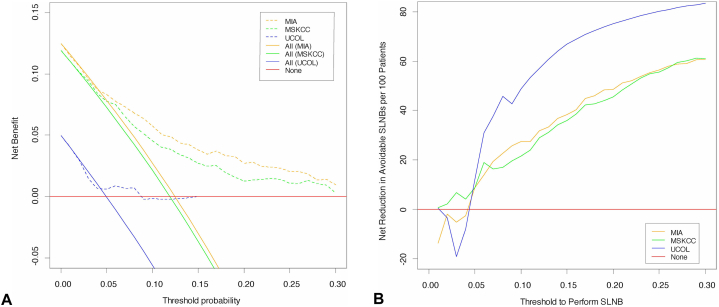
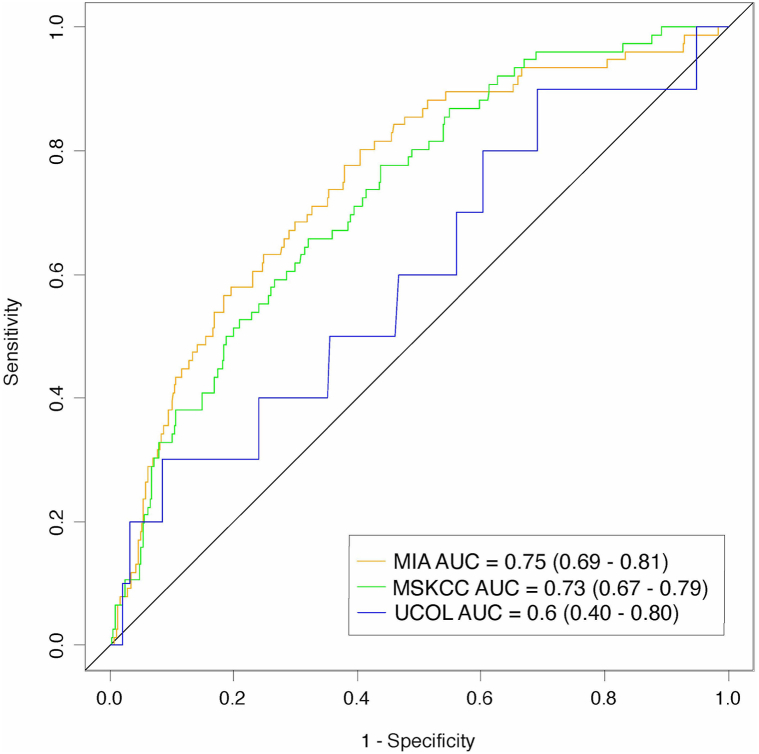
In this prognostic validation, statistical accuracy was assessed through discrimination, measured with receiver operating characteristic curves and calibration plots. Clinical utility was evaluated via decision curve analysis to determine the net benefit and number of net avoidable interventions achieved with nomogram use.
Results
Among 712 melanoma cases included, model discrimination was highest for the MIA nomogram (C-statistic = 0.753; 95% confidence interval = 0.694-0.812), followed by MSKCC (0.729[0.671-0.787]), and University of Colorado (0.601[0.405-0.793]). The MIA and MSKCC nomograms were well-calibrated across clinically relevant risk thresholds. All nomograms achieved a net benefit and net reduction in avoidable SLNBs for risk thresholds ≥5%. There was minimal to no reduction in unnecessary interventions at age extremes (<50 and ≥ 80 years old) for specific risk strata and nomograms.
Limitations
This a 5-year retrospective study.
Conclusions
These nomograms can be used to support SLNB decision-making in this population but necessitate caution in patients at age extremes when used to reduce avoidable interventions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


