Boaz Karmazyn, Matthew M Jones, Lisa R Delaney, Ralph A Hicks, Ann E Freshour, Megan B Marine, Shannon L Thompson, S Gregory Jennings, George J Eckert, Monica M Forbes-Amrhein
{"title":"Costochondral junction variations in children younger than 2 years.","authors":"Boaz Karmazyn, Matthew M Jones, Lisa R Delaney, Ralph A Hicks, Ann E Freshour, Megan B Marine, Shannon L Thompson, S Gregory Jennings, George J Eckert, Monica M Forbes-Amrhein","doi":"10.1007/s00247-025-06316-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Costochondral junction fractures are considered specific for child abuse and typically heal with a deformed costochondral junction.</p><p><strong>Objective: </strong>To evaluate the types, location, and incidence of costochondral junction variations that can mimic fractures.</p><p><strong>Materials and methods: </strong>A 15-year retrospective study was conducted on children under 2 years of age who underwent chest and abdominal computerized tomography (CT) scans for pneumonia, fever, congenital lung disease, pain, or appendicitis. Randomized selection included 120 chest and 120 abdominal CT scans. Demographic and clinical information was obtained from medical record reviews. Two pediatric radiologists independently reviewed the studies and indicated the presence and location of costochondral junction variation patterns (spurs), and fissure, horizontal lucency, corner, or bucket handle as identified on two consecutive slices on axial views. Disagreements were resolved by a third radiologist. We excluded patients with underlying medical conditions that could affect the skeleton and studies with motion artifacts. A t-test was used to evaluate the relationships between age, CT slice thickness, and the diagnosis of costochondral junction variations. Kappa statistics were used to evaluate agreement.</p><p><strong>Results: </strong>A total of 123 children were excluded due to motion artifacts (n = 30), trauma (n = 31), being evaluated for child abuse (n = 3), slice thickness of 5 mm (n = 1), and underlying medical conditions (n = 58). The final group included 117 children (73 males and 44 females) with an average age of 1 year; 64 had chest and 53 abdominal CT scans. Agreement was fair (kappa = 0.29) at the patient level and poor at the rib level (kappa = 0-0.64). The final number of variations, after resolving disagreements with a third radiologist, was 46 of costochondral junction variations in 19 children (16.2%, 19/117); all were costochondral junction spurs at the levels of the second to eighth ribs. Costochondral junction variations were significantly more common in younger children (average 0.7 ± 0.6 years vs. 1.1 ± 0.6 years, P = 0.024) and when there was thinner CT slice thickness (average 1.6 ± 1.4 mm vs. 2.5 ± 1.5 mm, P = 0.041).</p><p><strong>Conclusion: </strong>Costochondral junction variations were identified in 16.2% of children under 2 years of age, and some may mimic healing costochondral junction fractures. There was only fair agreement between radiologists.</p>","PeriodicalId":19755,"journal":{"name":"Pediatric Radiology","volume":" ","pages":"1883-1890"},"PeriodicalIF":2.3000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12394368/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric Radiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00247-025-06316-0","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/17 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Costochondral junction fractures are considered specific for child abuse and typically heal with a deformed costochondral junction.
Objective: To evaluate the types, location, and incidence of costochondral junction variations that can mimic fractures.
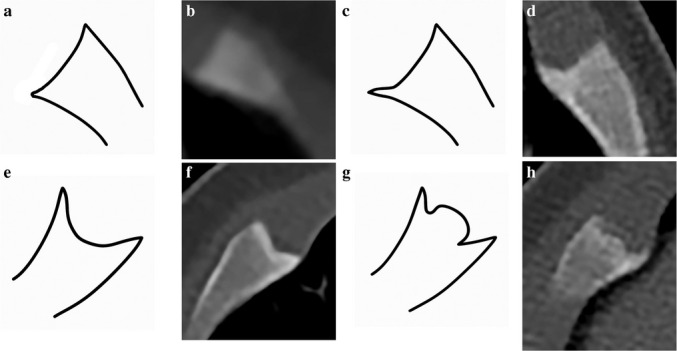
Materials and methods: A 15-year retrospective study was conducted on children under 2 years of age who underwent chest and abdominal computerized tomography (CT) scans for pneumonia, fever, congenital lung disease, pain, or appendicitis. Randomized selection included 120 chest and 120 abdominal CT scans. Demographic and clinical information was obtained from medical record reviews. Two pediatric radiologists independently reviewed the studies and indicated the presence and location of costochondral junction variation patterns (spurs), and fissure, horizontal lucency, corner, or bucket handle as identified on two consecutive slices on axial views. Disagreements were resolved by a third radiologist. We excluded patients with underlying medical conditions that could affect the skeleton and studies with motion artifacts. A t-test was used to evaluate the relationships between age, CT slice thickness, and the diagnosis of costochondral junction variations. Kappa statistics were used to evaluate agreement.
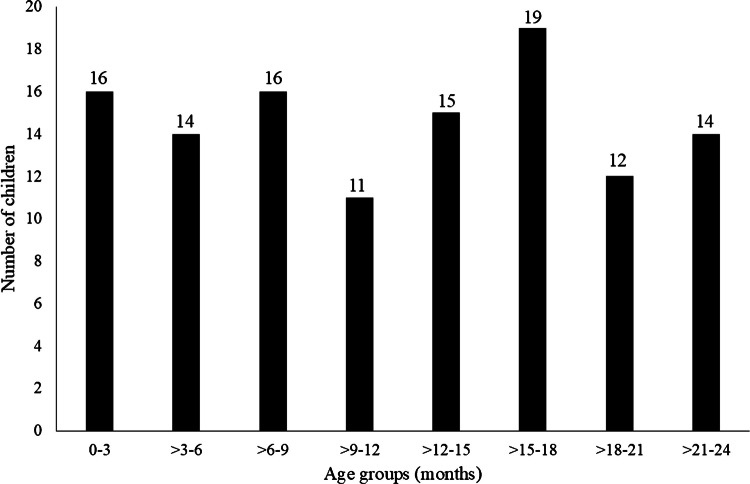
Results: A total of 123 children were excluded due to motion artifacts (n = 30), trauma (n = 31), being evaluated for child abuse (n = 3), slice thickness of 5 mm (n = 1), and underlying medical conditions (n = 58). The final group included 117 children (73 males and 44 females) with an average age of 1 year; 64 had chest and 53 abdominal CT scans. Agreement was fair (kappa = 0.29) at the patient level and poor at the rib level (kappa = 0-0.64). The final number of variations, after resolving disagreements with a third radiologist, was 46 of costochondral junction variations in 19 children (16.2%, 19/117); all were costochondral junction spurs at the levels of the second to eighth ribs. Costochondral junction variations were significantly more common in younger children (average 0.7 ± 0.6 years vs. 1.1 ± 0.6 years, P = 0.024) and when there was thinner CT slice thickness (average 1.6 ± 1.4 mm vs. 2.5 ± 1.5 mm, P = 0.041).
Conclusion: Costochondral junction variations were identified in 16.2% of children under 2 years of age, and some may mimic healing costochondral junction fractures. There was only fair agreement between radiologists.
期刊介绍:
Official Journal of the European Society of Pediatric Radiology, the Society for Pediatric Radiology and the Asian and Oceanic Society for Pediatric Radiology
Pediatric Radiology informs its readers of new findings and progress in all areas of pediatric imaging and in related fields. This is achieved by a blend of original papers, complemented by reviews that set out the present state of knowledge in a particular area of the specialty or summarize specific topics in which discussion has led to clear conclusions. Advances in technology, methodology, apparatus and auxiliary equipment are presented, and modifications of standard techniques are described.
Manuscripts submitted for publication must contain a statement to the effect that all human studies have been reviewed by the appropriate ethics committee and have therefore been performed in accordance with the ethical standards laid down in an appropriate version of the 1964 Declaration of Helsinki. It should also be stated clearly in the text that all persons gave their informed consent prior to their inclusion in the study. Details that might disclose the identity of the subjects under study should be omitted.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


