Abhinav R Balu, Rohan Bhargava, Mehul Mittal, Rachel Bergman, Milap Patel, Anish R Kadakia, Muhammad Mutawakkil
{"title":"Cost-Effectiveness of Locking vs Nonlocking Plates for Ankle Fracture Fixation: A Retrospective PROMIS-Based Cohort Study.","authors":"Abhinav R Balu, Rohan Bhargava, Mehul Mittal, Rachel Bergman, Milap Patel, Anish R Kadakia, Muhammad Mutawakkil","doi":"10.1177/24730114251351632","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The choice between locking and nonlocking plates for ankle fracture fixation is guided by implant cost, patient factors, fracture morphology, and clinical outcomes. Locking plates offer increased stability, particularly in osteopenic bone, and are available in low-profile, anatomically precontoured designs, though they are generally less malleable than nonlocking plates and are associated with higher cost. This study evaluates the cost-effectiveness of these methods by PROMIS (Patient-Reported Outcomes Measurement Information System) scores and complication rates. The primary outcome was defined as postoperative PROMIS pain interference and physical function scores.</p><p><strong>Methods: </strong>We conducted a retrospective review of ankle fracture fixations at our institution from 2016 to 2021. Surgical cost, outcome, and complication data were obtained through chart reviews. PROMIS scores were collected via structured telephonic interviews. PROMIS scores were analyzed with 2-sided <i>t</i> tests (Python 3.11.4, SciPy). Complication rates were evaluated with χ<sup>2</sup> tests (Python 3.11.4, statsmodels).</p><p><strong>Results: </strong>Of 493 patients, 283 received locking plate fixation and 210 nonlocking. Locking plate fixations cost 3.61 (95% CI: 2.81-4.64) times as much as nonlocking plate fixations, and reoperations cost 4.15 (95% CI: 1.11-15.47) times more. PROMIS pain interference and physical function scores did not differ significantly. Complications requiring reoperation occurred in 17.31% of locking plate patients and 21.9% of nonlocking plate patients (<i>P</i> = .20). Hardware removal occurred more often in the nonlocking group (<i>P</i> < .001), whereas infection was more frequent with locking plates (<i>P</i> < .05).</p><p><strong>Conclusion: </strong>Locking plates are significantly more expensive than nonlocking plates and did not demonstrate statistically significant differences in union rates, complication rates, or PROMIS scores between patients in this retrospective cohort. However, nonlocking plates had higher rates of uncomplicated syndesmotic screw removal rate whereas locking plates were associated with increased deep infection, resulting in a greater cost of reoperation compared with nonlocking plates. Although conclusions are limited by the study's retrospective nature and a significantly greater proportion of elderly and female patients in the locking plate cohort, it appears to demonstrate similar PROMIS scores and union rates outcomes.</p><p><strong>Level of evidence: </strong>Level III, retrospective cohort study.</p>","PeriodicalId":12429,"journal":{"name":"Foot & Ankle Orthopaedics","volume":"10 3","pages":"24730114251351632"},"PeriodicalIF":0.0000,"publicationDate":"2025-07-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12267897/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Foot & Ankle Orthopaedics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/24730114251351632","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The choice between locking and nonlocking plates for ankle fracture fixation is guided by implant cost, patient factors, fracture morphology, and clinical outcomes. Locking plates offer increased stability, particularly in osteopenic bone, and are available in low-profile, anatomically precontoured designs, though they are generally less malleable than nonlocking plates and are associated with higher cost. This study evaluates the cost-effectiveness of these methods by PROMIS (Patient-Reported Outcomes Measurement Information System) scores and complication rates. The primary outcome was defined as postoperative PROMIS pain interference and physical function scores.
Methods: We conducted a retrospective review of ankle fracture fixations at our institution from 2016 to 2021. Surgical cost, outcome, and complication data were obtained through chart reviews. PROMIS scores were collected via structured telephonic interviews. PROMIS scores were analyzed with 2-sided t tests (Python 3.11.4, SciPy). Complication rates were evaluated with χ2 tests (Python 3.11.4, statsmodels).
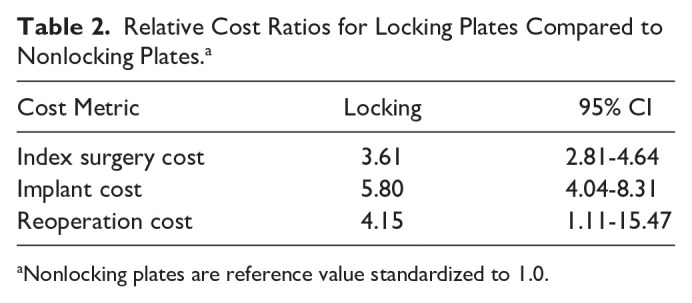
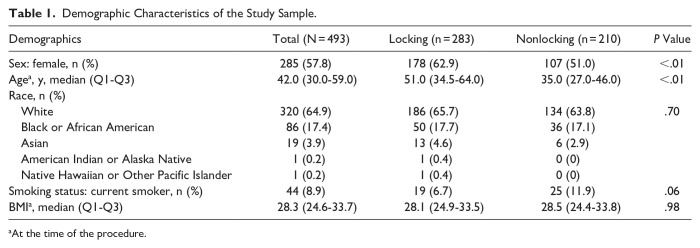
Results: Of 493 patients, 283 received locking plate fixation and 210 nonlocking. Locking plate fixations cost 3.61 (95% CI: 2.81-4.64) times as much as nonlocking plate fixations, and reoperations cost 4.15 (95% CI: 1.11-15.47) times more. PROMIS pain interference and physical function scores did not differ significantly. Complications requiring reoperation occurred in 17.31% of locking plate patients and 21.9% of nonlocking plate patients (P = .20). Hardware removal occurred more often in the nonlocking group (P < .001), whereas infection was more frequent with locking plates (P < .05).
Conclusion: Locking plates are significantly more expensive than nonlocking plates and did not demonstrate statistically significant differences in union rates, complication rates, or PROMIS scores between patients in this retrospective cohort. However, nonlocking plates had higher rates of uncomplicated syndesmotic screw removal rate whereas locking plates were associated with increased deep infection, resulting in a greater cost of reoperation compared with nonlocking plates. Although conclusions are limited by the study's retrospective nature and a significantly greater proportion of elderly and female patients in the locking plate cohort, it appears to demonstrate similar PROMIS scores and union rates outcomes.
Level of evidence: Level III, retrospective cohort study.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


