{"title":"A Case of Hemorrhagic Shock for a Ruptured Splenic Aneurysm Treated With REBOA-Assisted Surgery.","authors":"Chiara D'Alterio, Cristina Carruezzo, Armando Raso, Arezia Di Martino, Roberto Santoro, Domenico Giannotti","doi":"10.1155/cris/7264596","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Resuscitative endovascular balloon occlusion of the aorta (REBOA) is a technique aimed at temporarily interrupting or limiting blood flow through the aorta, which may be used as a bridge until definitive bleeding control by endovascular procedures or surgery. Despite the main current indication for its use is traumatic massive noncompressible torso hemorrhage, its application in end-stage nontraumatic abdominal and pelvic hemorrhage is progressively increasing. <b>Case Presentation:</b> A 42 year-old male patient was brought to our hospital Emergency Department with acute onset of abdominal pain, hypotension, paleness, and diaphoresis. A computed tomography (CT) was performed evidencing a voluminous retroperitoneal hematoma caused by the rupture of an unknown splenic aneurysm. Emergency open splenectomy with resection of the splenic aneurysm and evacuation of the retroperitoneal hematoma was performed, with the assistance of the REBOA technique. The endovascular balloon was positioned in the aorta, proximally to the celiac axis (Zone 1), through a percutaneous femoral access by the interventional radiologist. Intermittent aortic occlusion enabled proximal bleeding control, adequate myocardial and cerebral perfusion, and allowed surgeons to safely and successfully perform splenectomy by resecting the splenic artery at the origin. <b>Conclusion:</b> REBOA provides a rapid and minimally invasive hemodynamic control in severe hemorrhagic settings and its application in the initial management of nontraumatic abdominal hemorrhage should be strongly advised. Further studies with large sample size focusing on nontrauma patients are needed.</p>","PeriodicalId":9600,"journal":{"name":"Case Reports in Surgery","volume":"2025 ","pages":"7264596"},"PeriodicalIF":0.5000,"publicationDate":"2025-07-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12267891/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/cris/7264596","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
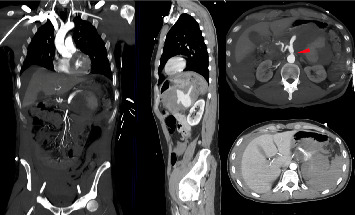
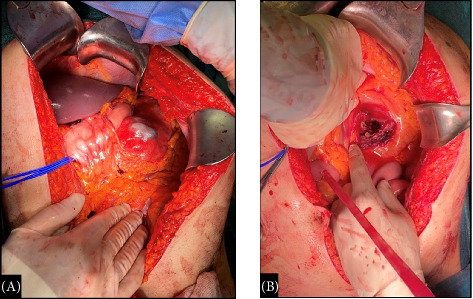
Background: Resuscitative endovascular balloon occlusion of the aorta (REBOA) is a technique aimed at temporarily interrupting or limiting blood flow through the aorta, which may be used as a bridge until definitive bleeding control by endovascular procedures or surgery. Despite the main current indication for its use is traumatic massive noncompressible torso hemorrhage, its application in end-stage nontraumatic abdominal and pelvic hemorrhage is progressively increasing. Case Presentation: A 42 year-old male patient was brought to our hospital Emergency Department with acute onset of abdominal pain, hypotension, paleness, and diaphoresis. A computed tomography (CT) was performed evidencing a voluminous retroperitoneal hematoma caused by the rupture of an unknown splenic aneurysm. Emergency open splenectomy with resection of the splenic aneurysm and evacuation of the retroperitoneal hematoma was performed, with the assistance of the REBOA technique. The endovascular balloon was positioned in the aorta, proximally to the celiac axis (Zone 1), through a percutaneous femoral access by the interventional radiologist. Intermittent aortic occlusion enabled proximal bleeding control, adequate myocardial and cerebral perfusion, and allowed surgeons to safely and successfully perform splenectomy by resecting the splenic artery at the origin. Conclusion: REBOA provides a rapid and minimally invasive hemodynamic control in severe hemorrhagic settings and its application in the initial management of nontraumatic abdominal hemorrhage should be strongly advised. Further studies with large sample size focusing on nontrauma patients are needed.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


