Comparison of bacterial colonization of implant abutment internal recess in internal hex and conical connection implants: An in vivo prospective study.
{"title":"Comparison of bacterial colonization of implant abutment internal recess in internal hex and conical connection implants: An in vivo prospective study.","authors":"Lalit Kumar, Shefali Singla, Jyoti Sharma, Komal Sehgal, Dhananjay Arora, Mili Gupta","doi":"10.4103/jips.jips_49_25","DOIUrl":null,"url":null,"abstract":"<p><strong>Aim: </strong>Microbial assessment of internal recess of two different internal implant connections in an in vivo study.</p><p><strong>Study settings and design: </strong>This randomized, in vivo study included 40 patients requiring mandibular single-tooth implant-supported prostheses, allocated into two equal groups based on implant connection design.</p><p><strong>Materials and methods: </strong>Group Internal Hex (IH) and group Conical Connection (CC) received implants with IH and CC, respectively. On the day of prosthetic loading, peri-implant sulcular fluid (PISF) sample was collected and stored. PISF samples were recollected after 3 months. Subsequently, the screw access hole was exposed, and the abutment screw was removed. Implant-abutment recess was washed with saline, lavage was sent for microbiological assay. The abutment screw and crown were restored. PISF was analyzed for interleukin-6 (IL-6).</p><p><strong>Statistical analysis used: </strong>For nonparametric values Chi square test and for parametric values t-test was used to analyse the data.</p><p><strong>Results: </strong>No implant failure or patient fallout was observed. In Group IH, 17 out of 20 samples were positive for aerobic viz-a-viz 7 samples from Group CC; P = 0.001. For anaerobic bacteria, similar results were obtained with a number of positive samples 19 as compared to 6 in respective groups; P = 0.00002. IL-6 values did not differ significantly from baseline to 3 months in either group.</p><p><strong>Conclusion: </strong>Within the limitations of the study, results show higher bacterial contamination of implant recess in IH than CC. However, the bacterial load had an insignificant contribution to IL-6 levels in PISF of the patients of either group in this time period.</p>","PeriodicalId":22669,"journal":{"name":"The Journal of Indian Prosthodontic Society","volume":"25 3","pages":"229-234"},"PeriodicalIF":1.0000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12370088/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Journal of Indian Prosthodontic Society","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/jips.jips_49_25","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/16 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"DENTISTRY, ORAL SURGERY & MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Aim: Microbial assessment of internal recess of two different internal implant connections in an in vivo study.
Study settings and design: This randomized, in vivo study included 40 patients requiring mandibular single-tooth implant-supported prostheses, allocated into two equal groups based on implant connection design.
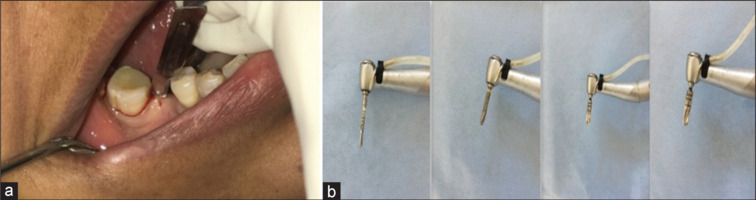
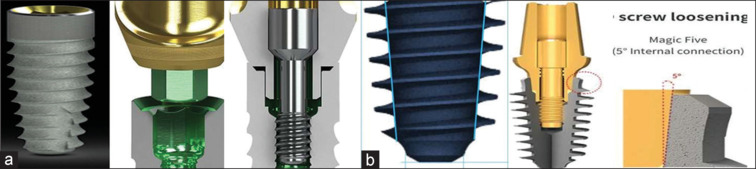
Materials and methods: Group Internal Hex (IH) and group Conical Connection (CC) received implants with IH and CC, respectively. On the day of prosthetic loading, peri-implant sulcular fluid (PISF) sample was collected and stored. PISF samples were recollected after 3 months. Subsequently, the screw access hole was exposed, and the abutment screw was removed. Implant-abutment recess was washed with saline, lavage was sent for microbiological assay. The abutment screw and crown were restored. PISF was analyzed for interleukin-6 (IL-6).
Statistical analysis used: For nonparametric values Chi square test and for parametric values t-test was used to analyse the data.
Results: No implant failure or patient fallout was observed. In Group IH, 17 out of 20 samples were positive for aerobic viz-a-viz 7 samples from Group CC; P = 0.001. For anaerobic bacteria, similar results were obtained with a number of positive samples 19 as compared to 6 in respective groups; P = 0.00002. IL-6 values did not differ significantly from baseline to 3 months in either group.
Conclusion: Within the limitations of the study, results show higher bacterial contamination of implant recess in IH than CC. However, the bacterial load had an insignificant contribution to IL-6 levels in PISF of the patients of either group in this time period.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


