Floor Nh Wilting, Lotte Sondag, Floris Hbm Schreuder, Ruben Dammers, Catharina Jm Klijn, Hieronymus D Boogaarts
{"title":"Surgery for spontaneous supratentorial intracerebral haemorrhage.","authors":"Floor Nh Wilting, Lotte Sondag, Floris Hbm Schreuder, Ruben Dammers, Catharina Jm Klijn, Hieronymus D Boogaarts","doi":"10.1002/14651858.CD015387.pub2","DOIUrl":null,"url":null,"abstract":"<p><strong>Rationale: </strong>It is unknown whether surgery improves outcomes in people with spontaneous supratentorial intracerebral haemorrhage (ICH), and whether the effects of surgery differ according to the applied surgical technique. This review updated the methodology of a previous Cochrane review from 2008.</p><p><strong>Objectives: </strong>To assess the benefits and harms of surgery plus standard medical management, compared to standard medical management alone, in people with spontaneous supratentorial ICH, and to assess whether the effect of surgery differs according to the surgical technique used.</p><p><strong>Search methods: </strong>We searched Cochrane Stroke Group Trials Register, CENTRAL, MEDLINE, and five other databases to 11 March 2025. We handsearched reference lists of included studies and relevant systematic reviews, forward-tracked relevant references, and contacted trialists for additional information on unpublished or ongoing studies.</p><p><strong>Eligibility criteria: </strong>We included randomised controlled trials (RCTs) of surgery (craniotomy with haematoma evacuation, minimally invasive surgery (MIS), or decompressive craniectomy) plus standard medical management in adults with a spontaneous supratentorial ICH, compared with standard medical management alone. We excluded studies of people with secondary causes of ICH (such as trauma, a macrovascular cause, or an intracranial tumour).</p><p><strong>Outcomes: </strong>Critical outcomes were: good functional outcome at end of scheduled follow-up, and all-cause mortality at end of scheduled follow-up. Important outcomes were: 30-day case fatality and health-related quality of life (HRQoL) at end of scheduled follow-up.</p><p><strong>Risk of bias: </strong>We used the Cochrane RoB 1 tool.</p><p><strong>Synthesis methods: </strong>We conducted meta-analyses using random-effects models to calculate risk ratios (RR) with 95% confidence intervals (CI) for dichotomous data, and mean differences (MD) with 95% CI for continuous data. We summarised the certainty of the evidence using GRADE.</p><p><strong>Included studies: </strong>We included 24 RCTs (4597 participants). The studies were conducted in Europe, North and South America, Asia, Africa, and Australia, and were published between 1989 and 2024. Twenty-three studies examined surgery aimed at clot removal plus standard medical management versus standard medical management, of which six were included in the separate comparison of craniotomy with haematoma evacuation plus standard medical management versus standard medical management, and 14 in the comparison of MIS plus standard medical management versus standard medical management. One study examined decompressive craniectomy without haematoma evacuation plus standard medical management versus standard medical management.</p><p><strong>Synthesis of results: </strong>Surgery aimed at clot removal plus standard medical management versus standard medical management alone Low-certainty evidence suggests that surgery aimed at clot removal may increase the chance of good functional outcome (RR 1.30, 95% CI 1.15 to 1.47; 18 studies, 4043 participants), and may reduce all-cause mortality (RR 0.79, 95% CI 0.71 to 0.88; 22 studies, 4278 participants) and 30-day case fatality (RR 0.74, 95% CI 0.60 to 0.90; 11 studies, 3179 participants). Surgery aimed at clot removal may have little to no effect on HRQoL, but the evidence is very uncertain (MD 0.03, 95% CI -0.05 to 0.11; 2 studies, 472 participants). Craniotomy with haematoma evacuation plus standard medical management versus standard medical management alone Craniotomy with haematoma evacuation may increase the chance of good functional outcome, but the evidence is very uncertain (RR 1.41, 95% CI 0.77 to 2.55; 6 studies, 853 participants). Craniotomy with haematoma evacuation likely reduces all-cause mortality (RR 0.80, 95% CI 0.67 to 0.96; 5 studies, 845 participants; moderate-certainty evidence), and may reduce 30-day case fatality (RR 0.68, 95% CI 0.46 to 1.00; 3 studies, 676 participants; low-certainty evidence), but the pooled CIs of 30-day case fatality included the possibility of no effect. Craniotomy with haematoma evacuation may result in little to no difference in HRQoL (MD 0.04, 95% CI -0.04 to 0.12; 1 study, 445 participants; low-certainty evidence). Minimally invasive surgery plus standard medical management versus standard medical management alone MIS may increase the chance of good functional outcome (RR 1.36, 95% CI 1.18 to 1.58; 10 studies, 2218 participants; low-certainty evidence), and probably reduces all-cause mortality (RR 0.71, 95% CI 0.60 to 0.84; 14 studies, 2401 participants; moderate-certainty evidence) and 30-day case fatality (RR 0.62, 95% CI 0.47 to 0.81; 7 studies, 1521 participants; moderate-certainty evidence). The evidence is very uncertain about HRQoL (MD -0.14, 95% CI -0.50 to 0.22; 1 study, 27 participants). Decompressive craniectomy plus standard medical management versus standard medical management alone Based on low-certainty evidence from one study, decompressive craniectomy may increase the chance of good functional outcome (RR 1.23, 95% CI 0.65 to 2.32; 182 participants), may reduce all-cause mortality (RR 0.74, 95% CI 0.45 to 1.19; 197 participants), and may result in little to no difference in HRQoL (MD 0.01, 95% CI -0.13 to 0.14), but the pooled CIs for these outcomes included the possibility of both benefit and harm. Decompressive craniectomy may also reduce 30-day case fatality, but the pooled CIs included the possibility of no effect (RR 0.43, 95% CI 0.19 to 1.00; 197 participants; low-certainty evidence).</p><p><strong>Authors' conclusions: </strong>For people with spontaneous supratentorial ICH, surgery aimed at clot removal may increase the chance of achieving good functional outcome and may reduce all-cause mortality and 30-day case fatality compared to standard medical management. When the results are divided by neurosurgical approach for haematoma evacuation, craniotomy likely reduces all-cause mortality and may reduce 30-day case fatality, while its effect on good functional outcome is very uncertain. MIS may increase the chance of good functional outcome, and probably reduces all-cause mortality and 30-day case fatality. Although the effect estimates for all outcomes regarding decompressive craniectomy may suggest a beneficial effect, the pooled estimates were very imprecise and included the possibility of a harmful (good functional outcome and all-cause mortality) or no effect (30-day case fatality). Evidence on HRQoL was low or very low certainty, overall, and for each surgical technique. The certainty of the evidence was limited due to methodological shortcomings and the high risk of bias of most included studies, as well as imprecise pooled estimates and substantial heterogeneity in some analyses. More high-quality and adequately powered studies are needed to be more certain and to guide clinical practice.</p><p><strong>Funding: </strong>This Cochrane review had no dedicated funding.</p><p><strong>Registration: </strong>Protocol (2022) available via doi.org/10.1002/14651858.CD015387.</p>","PeriodicalId":10473,"journal":{"name":"Cochrane Database of Systematic Reviews","volume":"7 ","pages":"CD015387"},"PeriodicalIF":8.8000,"publicationDate":"2025-07-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12269361/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cochrane Database of Systematic Reviews","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/14651858.CD015387.pub2","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Rationale: It is unknown whether surgery improves outcomes in people with spontaneous supratentorial intracerebral haemorrhage (ICH), and whether the effects of surgery differ according to the applied surgical technique. This review updated the methodology of a previous Cochrane review from 2008.
Objectives: To assess the benefits and harms of surgery plus standard medical management, compared to standard medical management alone, in people with spontaneous supratentorial ICH, and to assess whether the effect of surgery differs according to the surgical technique used.
Search methods: We searched Cochrane Stroke Group Trials Register, CENTRAL, MEDLINE, and five other databases to 11 March 2025. We handsearched reference lists of included studies and relevant systematic reviews, forward-tracked relevant references, and contacted trialists for additional information on unpublished or ongoing studies.
Eligibility criteria: We included randomised controlled trials (RCTs) of surgery (craniotomy with haematoma evacuation, minimally invasive surgery (MIS), or decompressive craniectomy) plus standard medical management in adults with a spontaneous supratentorial ICH, compared with standard medical management alone. We excluded studies of people with secondary causes of ICH (such as trauma, a macrovascular cause, or an intracranial tumour).
Outcomes: Critical outcomes were: good functional outcome at end of scheduled follow-up, and all-cause mortality at end of scheduled follow-up. Important outcomes were: 30-day case fatality and health-related quality of life (HRQoL) at end of scheduled follow-up.
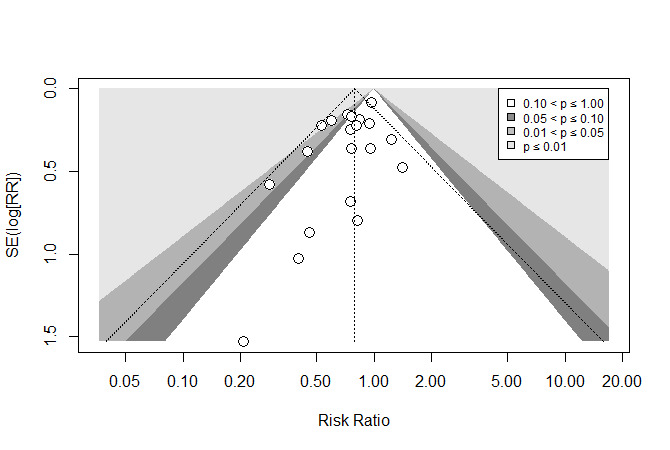
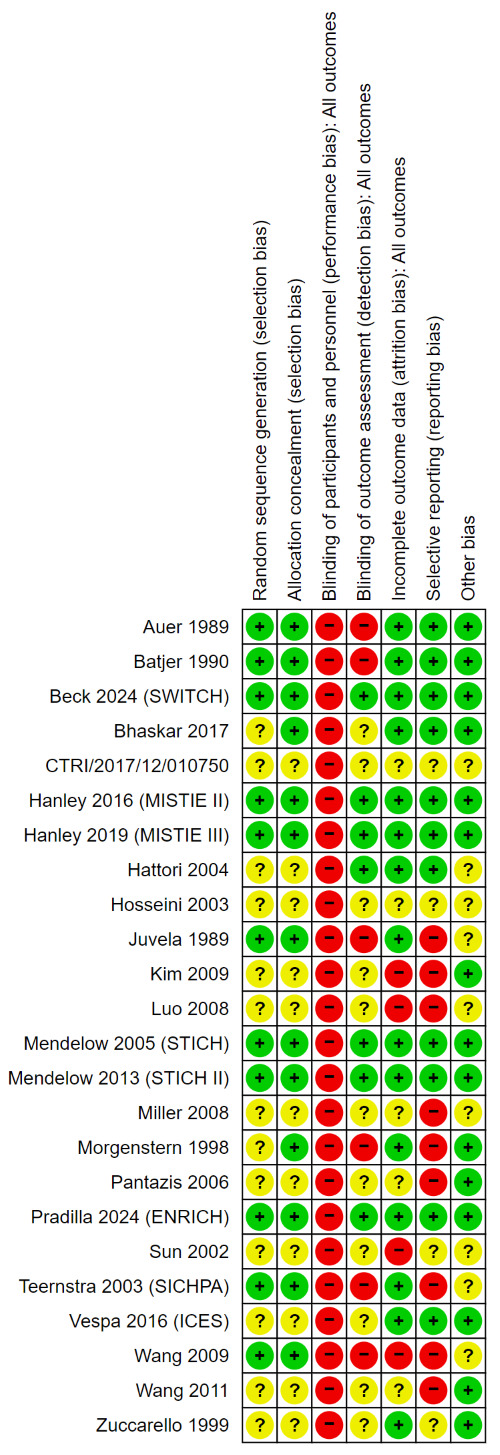
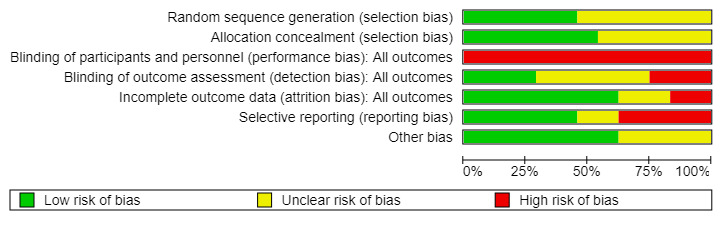
Risk of bias: We used the Cochrane RoB 1 tool.
Synthesis methods: We conducted meta-analyses using random-effects models to calculate risk ratios (RR) with 95% confidence intervals (CI) for dichotomous data, and mean differences (MD) with 95% CI for continuous data. We summarised the certainty of the evidence using GRADE.
Included studies: We included 24 RCTs (4597 participants). The studies were conducted in Europe, North and South America, Asia, Africa, and Australia, and were published between 1989 and 2024. Twenty-three studies examined surgery aimed at clot removal plus standard medical management versus standard medical management, of which six were included in the separate comparison of craniotomy with haematoma evacuation plus standard medical management versus standard medical management, and 14 in the comparison of MIS plus standard medical management versus standard medical management. One study examined decompressive craniectomy without haematoma evacuation plus standard medical management versus standard medical management.
Synthesis of results: Surgery aimed at clot removal plus standard medical management versus standard medical management alone Low-certainty evidence suggests that surgery aimed at clot removal may increase the chance of good functional outcome (RR 1.30, 95% CI 1.15 to 1.47; 18 studies, 4043 participants), and may reduce all-cause mortality (RR 0.79, 95% CI 0.71 to 0.88; 22 studies, 4278 participants) and 30-day case fatality (RR 0.74, 95% CI 0.60 to 0.90; 11 studies, 3179 participants). Surgery aimed at clot removal may have little to no effect on HRQoL, but the evidence is very uncertain (MD 0.03, 95% CI -0.05 to 0.11; 2 studies, 472 participants). Craniotomy with haematoma evacuation plus standard medical management versus standard medical management alone Craniotomy with haematoma evacuation may increase the chance of good functional outcome, but the evidence is very uncertain (RR 1.41, 95% CI 0.77 to 2.55; 6 studies, 853 participants). Craniotomy with haematoma evacuation likely reduces all-cause mortality (RR 0.80, 95% CI 0.67 to 0.96; 5 studies, 845 participants; moderate-certainty evidence), and may reduce 30-day case fatality (RR 0.68, 95% CI 0.46 to 1.00; 3 studies, 676 participants; low-certainty evidence), but the pooled CIs of 30-day case fatality included the possibility of no effect. Craniotomy with haematoma evacuation may result in little to no difference in HRQoL (MD 0.04, 95% CI -0.04 to 0.12; 1 study, 445 participants; low-certainty evidence). Minimally invasive surgery plus standard medical management versus standard medical management alone MIS may increase the chance of good functional outcome (RR 1.36, 95% CI 1.18 to 1.58; 10 studies, 2218 participants; low-certainty evidence), and probably reduces all-cause mortality (RR 0.71, 95% CI 0.60 to 0.84; 14 studies, 2401 participants; moderate-certainty evidence) and 30-day case fatality (RR 0.62, 95% CI 0.47 to 0.81; 7 studies, 1521 participants; moderate-certainty evidence). The evidence is very uncertain about HRQoL (MD -0.14, 95% CI -0.50 to 0.22; 1 study, 27 participants). Decompressive craniectomy plus standard medical management versus standard medical management alone Based on low-certainty evidence from one study, decompressive craniectomy may increase the chance of good functional outcome (RR 1.23, 95% CI 0.65 to 2.32; 182 participants), may reduce all-cause mortality (RR 0.74, 95% CI 0.45 to 1.19; 197 participants), and may result in little to no difference in HRQoL (MD 0.01, 95% CI -0.13 to 0.14), but the pooled CIs for these outcomes included the possibility of both benefit and harm. Decompressive craniectomy may also reduce 30-day case fatality, but the pooled CIs included the possibility of no effect (RR 0.43, 95% CI 0.19 to 1.00; 197 participants; low-certainty evidence).
Authors' conclusions: For people with spontaneous supratentorial ICH, surgery aimed at clot removal may increase the chance of achieving good functional outcome and may reduce all-cause mortality and 30-day case fatality compared to standard medical management. When the results are divided by neurosurgical approach for haematoma evacuation, craniotomy likely reduces all-cause mortality and may reduce 30-day case fatality, while its effect on good functional outcome is very uncertain. MIS may increase the chance of good functional outcome, and probably reduces all-cause mortality and 30-day case fatality. Although the effect estimates for all outcomes regarding decompressive craniectomy may suggest a beneficial effect, the pooled estimates were very imprecise and included the possibility of a harmful (good functional outcome and all-cause mortality) or no effect (30-day case fatality). Evidence on HRQoL was low or very low certainty, overall, and for each surgical technique. The certainty of the evidence was limited due to methodological shortcomings and the high risk of bias of most included studies, as well as imprecise pooled estimates and substantial heterogeneity in some analyses. More high-quality and adequately powered studies are needed to be more certain and to guide clinical practice.
Funding: This Cochrane review had no dedicated funding.
Registration: Protocol (2022) available via doi.org/10.1002/14651858.CD015387.
期刊介绍:
The Cochrane Database of Systematic Reviews (CDSR) stands as the premier database for systematic reviews in healthcare. It comprises Cochrane Reviews, along with protocols for these reviews, editorials, and supplements. Owned and operated by Cochrane, a worldwide independent network of healthcare stakeholders, the CDSR (ISSN 1469-493X) encompasses a broad spectrum of health-related topics, including health services.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


