Bassem Al Hariri, Muhammad Sharif, Lujain Al-Emadi, Richard Shamoon, Memon Noor Illahi, Nabil S Mahmood, Muayad Kasim Khalid
{"title":"COVID-19 Induced Cholangiopathy: A Case Report.","authors":"Bassem Al Hariri, Muhammad Sharif, Lujain Al-Emadi, Richard Shamoon, Memon Noor Illahi, Nabil S Mahmood, Muayad Kasim Khalid","doi":"10.1159/000546723","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>COVID-19, although primarily a respiratory illness, has been linked to complications in multiple organ systems, including the liver. Proposed mechanisms for liver injury include direct viral cytopathic effects, systemic inflammation, hypoxia, and drug-induced liver injury (DILI). Moreover, post-COVID cholangiopathy is an emerging entity with features that may overlap with autoimmune phenomena.</p><p><strong>Case presentation: </strong>A 60-year-old male patient with multiple comorbidities presented with fever, chills, and cough for 1 day. In the emergency department, he tested positive for COVID-19 by PCR and his chest X-ray revealed features suggestive of pulmonary edema. The patient was intubated and admitted to the Medical Intensive Care Unit (MICU) for management of COVID-19 pneumonia with pulmonary edema. During hospitalization, he developed cardiac complications that required targeted management. Approximately 1 week after admission, his liver enzymes began to rise. Although drug-DILI was initially suspected and hepatotoxic medications were discontinued with the initiation of ursodeoxycholic acid (UDCA), the liver function tests (LFTs) remained elevated. Subsequent magnetic resonance cholangiopancreatography revealed periportal inflammation with intrahepatic biliary dilatation and stricturing, findings consistent with COVID-19 induced cholangiopathy. The UDCA dosage was doubled, resulting in gradual biochemical improvement; however, the patient ultimately discharged against medical advice.</p><p><strong>Conclusion: </strong>COVID-19-induced cholangiopathy is a rare but serious liver complication. Effective management requires a multidisciplinary team. Ongoing research is needed to better understand long-term liver effects and improve care strategies.</p>","PeriodicalId":9614,"journal":{"name":"Case Reports in Gastroenterology","volume":"19 1","pages":"519-526"},"PeriodicalIF":0.6000,"publicationDate":"2025-07-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12266703/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000546723","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: COVID-19, although primarily a respiratory illness, has been linked to complications in multiple organ systems, including the liver. Proposed mechanisms for liver injury include direct viral cytopathic effects, systemic inflammation, hypoxia, and drug-induced liver injury (DILI). Moreover, post-COVID cholangiopathy is an emerging entity with features that may overlap with autoimmune phenomena.
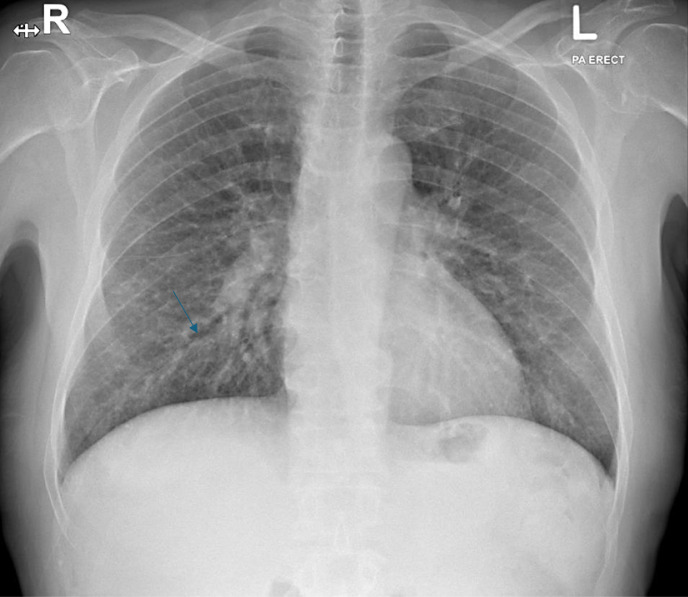
Case presentation: A 60-year-old male patient with multiple comorbidities presented with fever, chills, and cough for 1 day. In the emergency department, he tested positive for COVID-19 by PCR and his chest X-ray revealed features suggestive of pulmonary edema. The patient was intubated and admitted to the Medical Intensive Care Unit (MICU) for management of COVID-19 pneumonia with pulmonary edema. During hospitalization, he developed cardiac complications that required targeted management. Approximately 1 week after admission, his liver enzymes began to rise. Although drug-DILI was initially suspected and hepatotoxic medications were discontinued with the initiation of ursodeoxycholic acid (UDCA), the liver function tests (LFTs) remained elevated. Subsequent magnetic resonance cholangiopancreatography revealed periportal inflammation with intrahepatic biliary dilatation and stricturing, findings consistent with COVID-19 induced cholangiopathy. The UDCA dosage was doubled, resulting in gradual biochemical improvement; however, the patient ultimately discharged against medical advice.
Conclusion: COVID-19-induced cholangiopathy is a rare but serious liver complication. Effective management requires a multidisciplinary team. Ongoing research is needed to better understand long-term liver effects and improve care strategies.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


