2D-cranial T1-black-blood MRI in suspected giant cell arteritis-measurement of vessel wall thickness does not give a diagnostic advantage compared to visual scoring alone.
{"title":"2D-cranial T1-black-blood MRI in suspected giant cell arteritis-measurement of vessel wall thickness does not give a diagnostic advantage compared to visual scoring alone.","authors":"Pascal Seitz, Susana Bucher, Lukas Bütikofer, Britta Maurer, Harald Marcel Bonel, Fabian Lötscher, Luca Seitz","doi":"10.3389/fradi.2025.1597938","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To compare two established scoring schemes for the 2D-T1-weighted \"black-blood\" MRI sequence (T1-BB) for superficial cranial arteries (SCA) in the diagnosis of giant cell arteritis (GCA).</p><p><strong>Methods: </strong>Ten arterial segments were evaluated in T1-BB images with two different methods: a visual semiquantitative scheme (T1-BB-VISUAL) and a composite scheme that included both the semiquantitative assessment and a quantitative wall thickness measurement (T1-BB-COMP). The expert clinical diagnosis after ≥6 months of follow-up was the diagnostic reference standard. Diagnostic accuracy and agreement on the segment and patient levels were evaluated for the two different rating schemes.</p><p><strong>Results: </strong>Retrospectively, 151 consecutive patients with clinically suspected GCA were included. The study cohort consisted of 82 patients with and 69 without GCA. For the T1-BB-COMP and the T1-BB-VISUAL, the sensitivity was 81.7% vs. 87.8% (<i>p</i> = 0.025), the specificity was 91.3% vs. 88.4% (<i>p</i> = 0.16) and the proportion of correct diagnoses was 86.1% vs. 88.1% (<i>p</i> = 0.26), respectively. The overall agreement between the two methods for 1,201 rated arterial segments was very good at 91.6% with a kappa of 0.80. The agreement was higher for segments with a larger calibre than for smaller segments: common superficial temporal arteries 98.0%, occipital arteries 93.2%, frontal branches 89.8% and parietal branches 86.9%. The correlation of wall thickness measurements between readers was strong (Spearman's rho of 0.68). The time needed to apply the T1-BB-VISUAL was about half as long as for the T1-BB-COMP (4.5 vs. 8.95 minutes).</p><p><strong>Conclusion: </strong>In suspected GCA, the additional measurement of the wall thickness of SCAs in 2D-T1-BB MRI does not lead to a better diagnostic performance compared to visual semiquantitative scoring alone. Visual scoring is preferred due to higher efficiency and reliability.</p>","PeriodicalId":73101,"journal":{"name":"Frontiers in radiology","volume":"5 ","pages":"1597938"},"PeriodicalIF":2.3000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12260534/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in radiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3389/fradi.2025.1597938","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
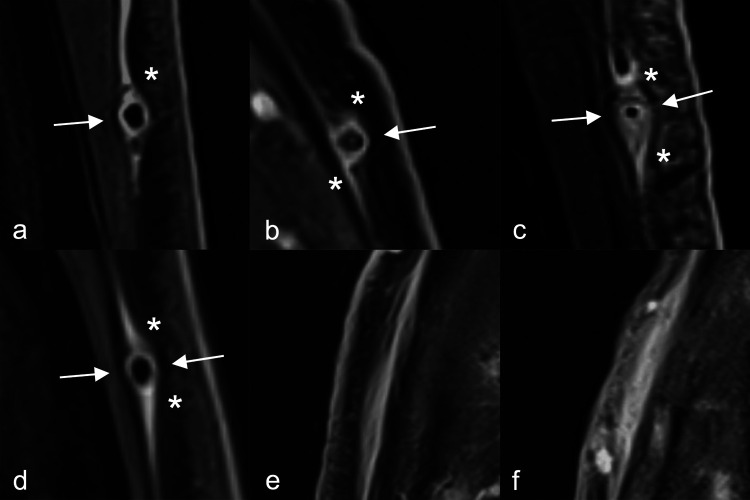
Objectives: To compare two established scoring schemes for the 2D-T1-weighted "black-blood" MRI sequence (T1-BB) for superficial cranial arteries (SCA) in the diagnosis of giant cell arteritis (GCA).
Methods: Ten arterial segments were evaluated in T1-BB images with two different methods: a visual semiquantitative scheme (T1-BB-VISUAL) and a composite scheme that included both the semiquantitative assessment and a quantitative wall thickness measurement (T1-BB-COMP). The expert clinical diagnosis after ≥6 months of follow-up was the diagnostic reference standard. Diagnostic accuracy and agreement on the segment and patient levels were evaluated for the two different rating schemes.
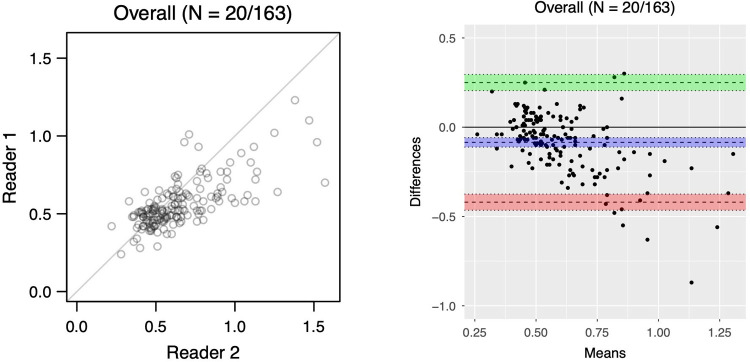
Results: Retrospectively, 151 consecutive patients with clinically suspected GCA were included. The study cohort consisted of 82 patients with and 69 without GCA. For the T1-BB-COMP and the T1-BB-VISUAL, the sensitivity was 81.7% vs. 87.8% (p = 0.025), the specificity was 91.3% vs. 88.4% (p = 0.16) and the proportion of correct diagnoses was 86.1% vs. 88.1% (p = 0.26), respectively. The overall agreement between the two methods for 1,201 rated arterial segments was very good at 91.6% with a kappa of 0.80. The agreement was higher for segments with a larger calibre than for smaller segments: common superficial temporal arteries 98.0%, occipital arteries 93.2%, frontal branches 89.8% and parietal branches 86.9%. The correlation of wall thickness measurements between readers was strong (Spearman's rho of 0.68). The time needed to apply the T1-BB-VISUAL was about half as long as for the T1-BB-COMP (4.5 vs. 8.95 minutes).
Conclusion: In suspected GCA, the additional measurement of the wall thickness of SCAs in 2D-T1-BB MRI does not lead to a better diagnostic performance compared to visual semiquantitative scoring alone. Visual scoring is preferred due to higher efficiency and reliability.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


