{"title":"[Treatment of oral lichen planus-a review].","authors":"Khava Abdusalamova, Farzan Solimani, Margitta Worm","doi":"10.1007/s00105-025-05540-x","DOIUrl":null,"url":null,"abstract":"<p><p>Mucosal lichen planus (MLP) is a chronic, recurrent, inflammatory T‑cell disorder that can affect mucous membranes and, together with cutaneous lichen planus (CLP) and lichen planopilaris (LPP), belongs to the variants of lichen planus (LP) diseases. MLP can affect both the oral mucosa (oral lichen planus, OLP) and the genital mucosa. Patients with OLP can have varying degrees of severity. In particular, patients affected by an erosive/ulcerative form usually pose a therapeutic challenge because 1) there are currently no US Food and Drug Administration(FDA)/European Medicines Agency (EMA)-approved drugs and 2) the disease is often treatment resistant. Recently published studies on immunopathogenesis describe a predominant role of interferon-γ-induced inflammation, but many aspects of the disease are still unknown. Accordingly, primarily symptomatic therapies are currently available. In addition to topical glucocorticoids, retinoids in topical and systemic form and systemic glucocorticoids are established first-line therapies. A wide range of second- and third-line therapies show that no standard treatment that there is still o standard treatment. Among the new therapies, Janus kinase inhibitors and monoclonal antibodies should be emphasized, as they could expand the therapeutic spectrum for OLP in the future. However, prospective, placebo-controlled studies are needed for this in the future. Alternative and complementary treatments such as herbal therapies, phototherapy, platelet-rich plasma (PRP) and injectable platelet-rich fibrin (i-PRF) are also described in the literature. In this article, we discuss the current therapeutic options for this difficult-to-treat disease.</p>","PeriodicalId":72786,"journal":{"name":"Dermatologie (Heidelberg, Germany)","volume":" ","pages":"491-498"},"PeriodicalIF":0.7000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12313821/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Dermatologie (Heidelberg, Germany)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s00105-025-05540-x","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/15 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
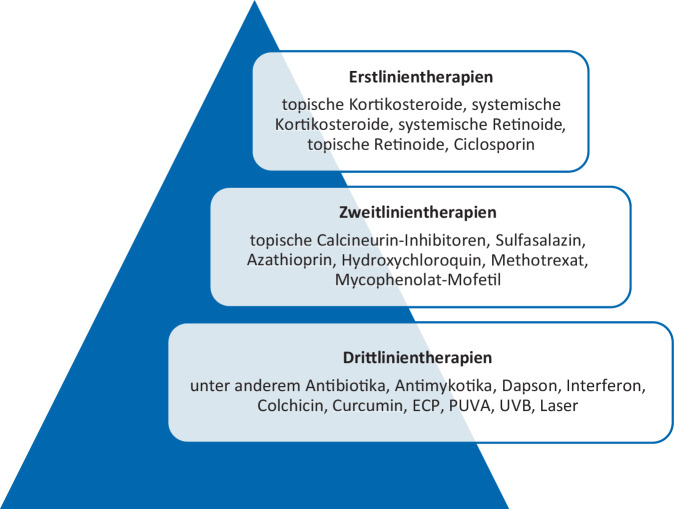
Mucosal lichen planus (MLP) is a chronic, recurrent, inflammatory T‑cell disorder that can affect mucous membranes and, together with cutaneous lichen planus (CLP) and lichen planopilaris (LPP), belongs to the variants of lichen planus (LP) diseases. MLP can affect both the oral mucosa (oral lichen planus, OLP) and the genital mucosa. Patients with OLP can have varying degrees of severity. In particular, patients affected by an erosive/ulcerative form usually pose a therapeutic challenge because 1) there are currently no US Food and Drug Administration(FDA)/European Medicines Agency (EMA)-approved drugs and 2) the disease is often treatment resistant. Recently published studies on immunopathogenesis describe a predominant role of interferon-γ-induced inflammation, but many aspects of the disease are still unknown. Accordingly, primarily symptomatic therapies are currently available. In addition to topical glucocorticoids, retinoids in topical and systemic form and systemic glucocorticoids are established first-line therapies. A wide range of second- and third-line therapies show that no standard treatment that there is still o standard treatment. Among the new therapies, Janus kinase inhibitors and monoclonal antibodies should be emphasized, as they could expand the therapeutic spectrum for OLP in the future. However, prospective, placebo-controlled studies are needed for this in the future. Alternative and complementary treatments such as herbal therapies, phototherapy, platelet-rich plasma (PRP) and injectable platelet-rich fibrin (i-PRF) are also described in the literature. In this article, we discuss the current therapeutic options for this difficult-to-treat disease.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


