Jim M Smit, Jasper Van Bommel, Diederik A M P J Gommers, Marcel J T Reinders, Michel E Van Genderen, Jesse H Krijthe, Annemijn H Jonkman
{"title":"Switching from controlled to assisted mechanical ventilation: a multi-center retrospective study (SWITCH).","authors":"Jim M Smit, Jasper Van Bommel, Diederik A M P J Gommers, Marcel J T Reinders, Michel E Van Genderen, Jesse H Krijthe, Annemijn H Jonkman","doi":"10.1186/s40635-025-00785-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Switching from controlled to assisted ventilation is crucial in the trajectory of intensive care unit (ICU) stay, but no guidelines exist. We described current practices, analyzed patient characteristics associated with switch success or failure, and explored the feasibility to predict switch failure.</p><p><strong>Methods: </strong>In this retrospective study, we obtained highly granular longitudinal ICU data sets from three medical centers, covering demographics, severity scores, vital signs, ventilation, and laboratory parameters. The primary endpoint was switch success, considering a switch attempt to be successful if a patient did not return to controlled ventilation for the next 72 h while alive, and to be failed otherwise. We compared the characteristics of patients with successful vs. failed first switch attempts at ICU admission, immediately before, and 3 h after the attempt. We trained LASSO logistic regression models to predict switch failure.</p><p><strong>Results: </strong>In 4524/6715 (67%) patients attempting a switch, the first attempt failed. The first switch attempt, regardless of success or failure, was generally made at normalized PaCO<sub>2</sub> and pH levels, with PEEP < 10 cmH<sub>2</sub>O and PaO<sub>2</sub>/FiO<sub>2</sub> indicating mild injury. Despite very similar baseline disease severity, switch failure was associated with significantly worse outcomes, including a 28-day mortality of 27% vs. 16% and median ventilator-free days of 16 vs. 22 (p < 0.001). Failed attempts were initiated significantly earlier than successful ones (median 1.8 vs. 1.3 days, p < 0.001). Before the switch, PaO<sub>2</sub>/FiO<sub>2</sub>, if measured at PEEP > 10 cmH<sub>2</sub>O, and respiratory system compliance was lower in patients with switch failure (median 185 vs. 205 mmHg, p < 0.001; 39 vs. 41 mL/cmH<sub>2</sub>O, P = 0.001), and post-switch, patients with switch failure experienced greater deterioration in gas exchange and minimal improvement in ventilatory parameters post-switch. Contrary to our hypotheses, patient characteristics for failed vs. successful switches were surprisingly similar, resulting in prediction models with limited discriminative performance.</p><p><strong>Conclusions: </strong>Approximately two-thirds of attempts to switch patients to assisted ventilation fail, which are associated with significantly worse clinical outcomes, despite similar baseline disease severity. Contrary to our hypotheses, patients with successful and failed attempts showed similar characteristics, making switch failure difficult to predict. These findings underscore the importance of preventing switch failures and, given the retrospective nature of this study, highlight the need for prospective studies to better understand the reasons for switch failure and when spontaneous breathing can be safely initiated.</p>","PeriodicalId":13750,"journal":{"name":"Intensive Care Medicine Experimental","volume":"13 1","pages":"73"},"PeriodicalIF":2.8000,"publicationDate":"2025-07-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12267752/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Intensive Care Medicine Experimental","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40635-025-00785-1","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Switching from controlled to assisted ventilation is crucial in the trajectory of intensive care unit (ICU) stay, but no guidelines exist. We described current practices, analyzed patient characteristics associated with switch success or failure, and explored the feasibility to predict switch failure.
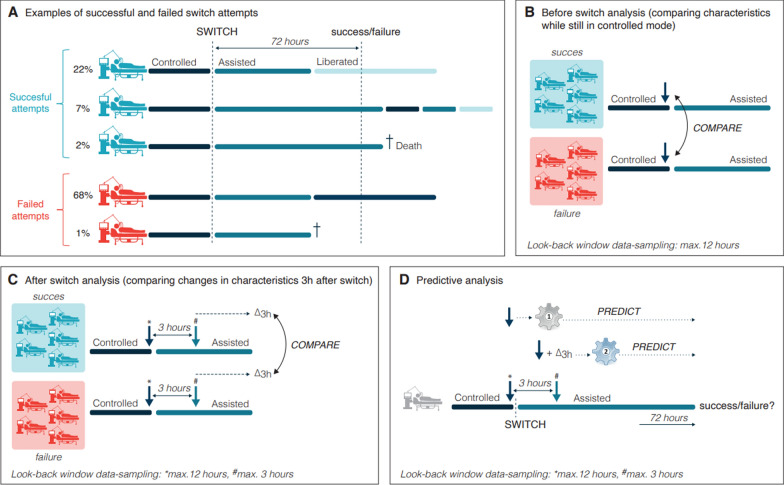
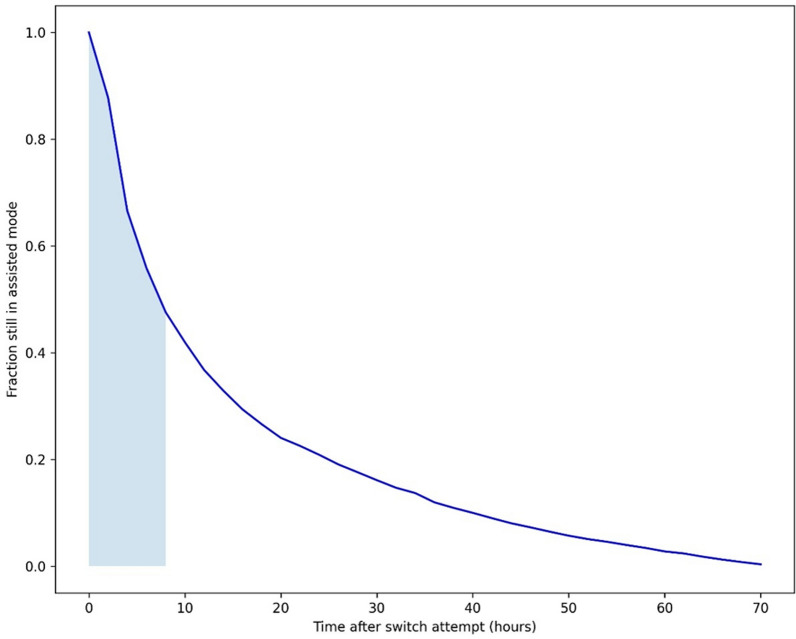
Methods: In this retrospective study, we obtained highly granular longitudinal ICU data sets from three medical centers, covering demographics, severity scores, vital signs, ventilation, and laboratory parameters. The primary endpoint was switch success, considering a switch attempt to be successful if a patient did not return to controlled ventilation for the next 72 h while alive, and to be failed otherwise. We compared the characteristics of patients with successful vs. failed first switch attempts at ICU admission, immediately before, and 3 h after the attempt. We trained LASSO logistic regression models to predict switch failure.
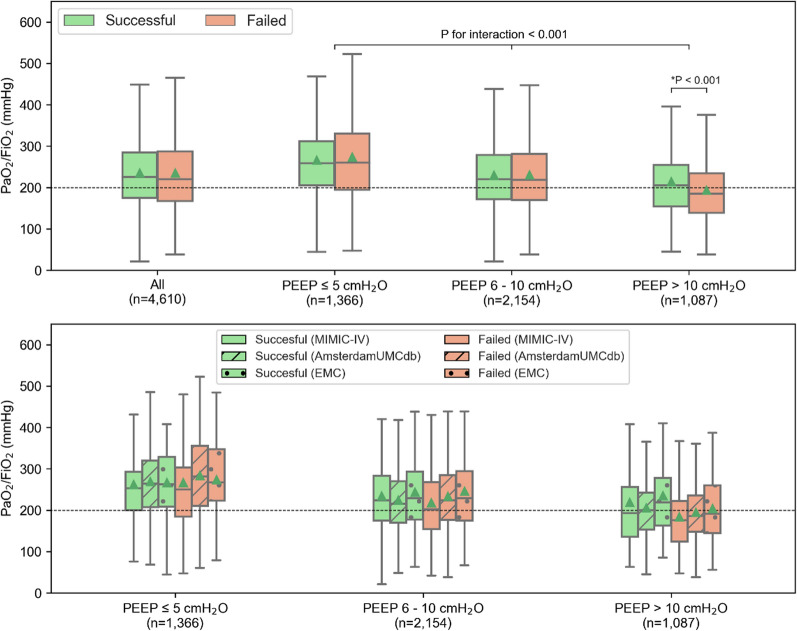
Results: In 4524/6715 (67%) patients attempting a switch, the first attempt failed. The first switch attempt, regardless of success or failure, was generally made at normalized PaCO2 and pH levels, with PEEP < 10 cmH2O and PaO2/FiO2 indicating mild injury. Despite very similar baseline disease severity, switch failure was associated with significantly worse outcomes, including a 28-day mortality of 27% vs. 16% and median ventilator-free days of 16 vs. 22 (p < 0.001). Failed attempts were initiated significantly earlier than successful ones (median 1.8 vs. 1.3 days, p < 0.001). Before the switch, PaO2/FiO2, if measured at PEEP > 10 cmH2O, and respiratory system compliance was lower in patients with switch failure (median 185 vs. 205 mmHg, p < 0.001; 39 vs. 41 mL/cmH2O, P = 0.001), and post-switch, patients with switch failure experienced greater deterioration in gas exchange and minimal improvement in ventilatory parameters post-switch. Contrary to our hypotheses, patient characteristics for failed vs. successful switches were surprisingly similar, resulting in prediction models with limited discriminative performance.
Conclusions: Approximately two-thirds of attempts to switch patients to assisted ventilation fail, which are associated with significantly worse clinical outcomes, despite similar baseline disease severity. Contrary to our hypotheses, patients with successful and failed attempts showed similar characteristics, making switch failure difficult to predict. These findings underscore the importance of preventing switch failures and, given the retrospective nature of this study, highlight the need for prospective studies to better understand the reasons for switch failure and when spontaneous breathing can be safely initiated.
背景:从受控通气到辅助通气的切换对重症监护病房(ICU)的住院轨迹至关重要,但目前尚无指南。我们描述了目前的做法,分析了与开关成功或失败相关的患者特征,并探讨了预测开关失败的可行性。方法:在这项回顾性研究中,我们从三个医疗中心获得了高度细化的ICU纵向数据集,包括人口统计学、严重程度评分、生命体征、通气和实验室参数。主要终点是切换成功,如果患者在接下来的72小时内未恢复受控通气,则考虑切换尝试成功,否则失败。我们比较了在ICU入院时、尝试前和尝试后3小时首次切换尝试成功与失败患者的特征。我们训练LASSO逻辑回归模型来预测开关故障。结果:在4524/6715(67%)患者中,第一次尝试失败。无论成功与否,第一次开关尝试通常是在正常的PaCO2和pH水平下进行的,PEEP 2O和PaO2/FiO2表示轻度损伤。尽管基线疾病严重程度非常相似,但开关失效与明显较差的结果相关,包括28天死亡率为27% vs. 16%,无呼吸机的中位天数为16 vs. 22 (p 2/FiO2,如果在PEEP > 10 cmH2O测量),开关失效患者的呼吸系统依从性较低(中位185 vs. 205 mmHg, p 2O, p = 0.001)。开关失败的患者在气体交换方面有更大的恶化,开关后通气参数的改善很小。与我们的假设相反,开关失败和成功的患者特征惊人地相似,导致预测模型的判别性能有限。结论:尽管基线疾病严重程度相似,但大约三分之二的患者尝试切换到辅助通气失败,这与明显更差的临床结果相关。与我们的假设相反,尝试成功和失败的患者表现出相似的特征,使得切换失败难以预测。这些发现强调了预防开关故障的重要性,并且鉴于本研究的回顾性性质,强调了前瞻性研究的必要性,以更好地了解开关故障的原因以及何时可以安全地启动自发呼吸。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


