Ori Aslan, Johnathan Arnon, Itamar Averbuch, Daniel Reinhorn, Hovav Nechushtan, Yakir Rottenberg, Philip Blumenfeld
{"title":"Planning Target Volume and Nodal Status Predict Clinical Outcomes After Chemoradiation and Durvalumab in Stage III Non-Small Cell Lung Cancer.","authors":"Ori Aslan, Johnathan Arnon, Itamar Averbuch, Daniel Reinhorn, Hovav Nechushtan, Yakir Rottenberg, Philip Blumenfeld","doi":"10.1111/1759-7714.70130","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Unresectable Stage III non-small cell lung cancer (NSCLC) presents a major clinical challenge due to its heterogeneous nature and poor prognosis. Despite aggressive treatment with concurrent chemoradiation (CRT) and the introduction of Durvalumab consolidation therapy, the risk of recurrence remains high, necessitating research into predictors of clinical outcomes.</p><p><strong>Methods: </strong>In this retrospective, two-center study, we reviewed cases of 141 patients with Stage III unresectable NSCLC, treated with CRT followed by Durvalumab between 2017 and 2023. We retrieved clinical and treatment characteristics and analyzed associations with clinical outcomes.</p><p><strong>Results: </strong>Utilizing a binary threshold for planning target volume (PTV), patients with PTV ≥ 350 cm<sup>3</sup> had significantly worse progression-free survival (PFS) compared to those with PTV < 350 cm<sup>3</sup>, with a median PFS of 16.2 months compared with 30.9 months, respectively, HR 1.78 (95% CI 1.14-2.68), p = 0.01. Nodal status was also associated with worse PFS, with patients having N3 disease exhibiting a median PFS of 5.1 months compared to 15.2 months for N0-N2 disease, HR 2.09 (95% CI 1.28-3.41), p = 0.003. PTV ≥ 350 cm<sup>3</sup> and N3 involvement remained significantly associated with PFS in multivariable analysis. Both variables were associated with early and distant recurrence patterns, and PTV ≥ 350 cm<sup>3</sup> was associated with worse survival.</p><p><strong>Conclusions: </strong>This study identifies PTV ≥ 350 cm<sup>3</sup> and nodal involvement as key predictors of worse clinical outcomes in patients with Stage III NSCLC treated with CRT and Durvalumab. The PTV threshold of 350 cm<sup>3</sup> provides a practical, clinically applicable tool for risk stratification that could guide intensification of treatment and surveillance to improve outcomes in high-risk patients.</p>","PeriodicalId":23338,"journal":{"name":"Thoracic Cancer","volume":"16 14","pages":"e70130"},"PeriodicalIF":2.3000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12260756/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Thoracic Cancer","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/1759-7714.70130","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Unresectable Stage III non-small cell lung cancer (NSCLC) presents a major clinical challenge due to its heterogeneous nature and poor prognosis. Despite aggressive treatment with concurrent chemoradiation (CRT) and the introduction of Durvalumab consolidation therapy, the risk of recurrence remains high, necessitating research into predictors of clinical outcomes.
Methods: In this retrospective, two-center study, we reviewed cases of 141 patients with Stage III unresectable NSCLC, treated with CRT followed by Durvalumab between 2017 and 2023. We retrieved clinical and treatment characteristics and analyzed associations with clinical outcomes.
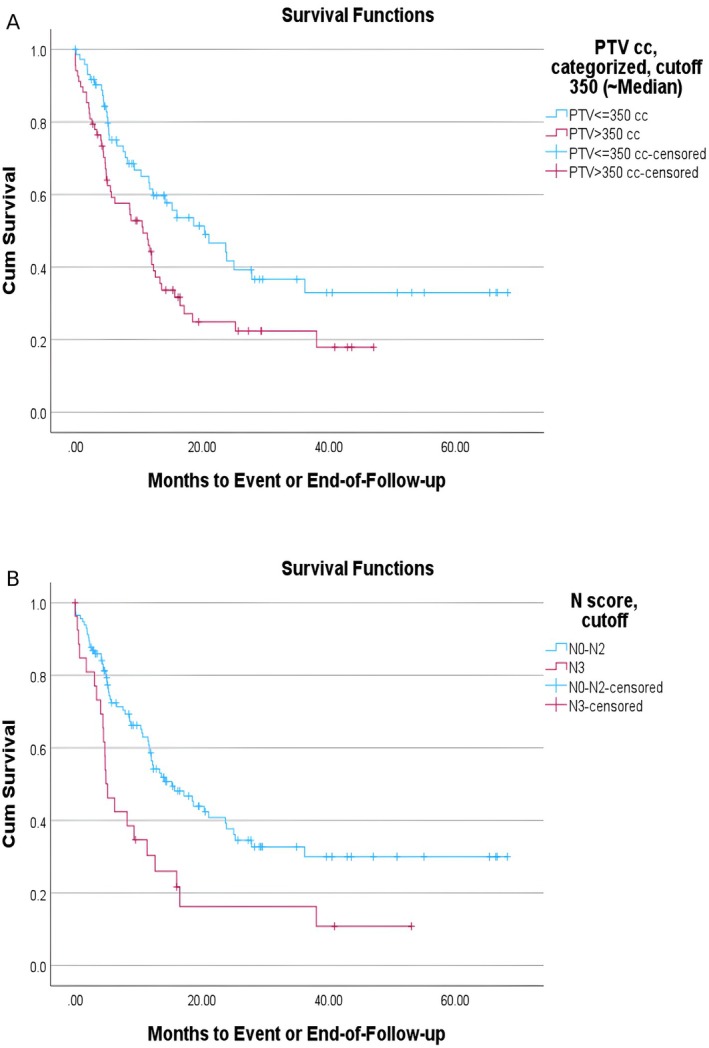
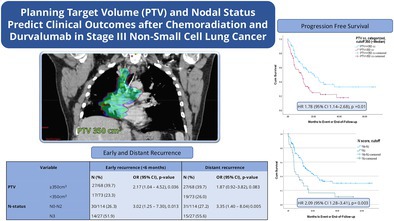
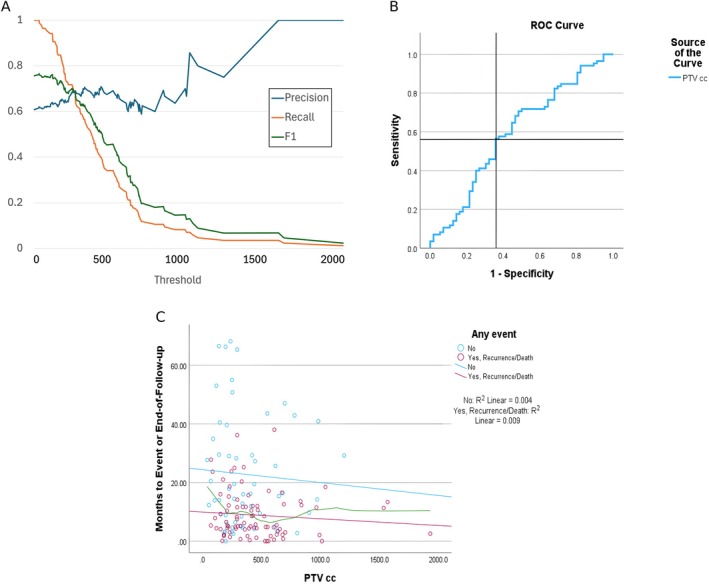
Results: Utilizing a binary threshold for planning target volume (PTV), patients with PTV ≥ 350 cm3 had significantly worse progression-free survival (PFS) compared to those with PTV < 350 cm3, with a median PFS of 16.2 months compared with 30.9 months, respectively, HR 1.78 (95% CI 1.14-2.68), p = 0.01. Nodal status was also associated with worse PFS, with patients having N3 disease exhibiting a median PFS of 5.1 months compared to 15.2 months for N0-N2 disease, HR 2.09 (95% CI 1.28-3.41), p = 0.003. PTV ≥ 350 cm3 and N3 involvement remained significantly associated with PFS in multivariable analysis. Both variables were associated with early and distant recurrence patterns, and PTV ≥ 350 cm3 was associated with worse survival.
Conclusions: This study identifies PTV ≥ 350 cm3 and nodal involvement as key predictors of worse clinical outcomes in patients with Stage III NSCLC treated with CRT and Durvalumab. The PTV threshold of 350 cm3 provides a practical, clinically applicable tool for risk stratification that could guide intensification of treatment and surveillance to improve outcomes in high-risk patients.
背景:不可切除的III期非小细胞肺癌(NSCLC)由于其异质性和预后差,是一个重大的临床挑战。尽管采用同步放化疗(CRT)进行积极治疗,并引入Durvalumab巩固治疗,但复发的风险仍然很高,需要对临床结果的预测因素进行研究。方法:在这项回顾性的双中心研究中,我们回顾了141例在2017年至2023年间接受CRT和Durvalumab治疗的III期不可切除NSCLC患者。我们检索了临床和治疗特征,并分析了与临床结果的关联。结果:利用二值阈值规划靶体积(PTV), PTV≥350 cm3的患者的无进展生存期(PFS)明显差于PTV为3的患者,中位PFS分别为16.2个月和30.9个月,HR为1.78 (95% CI 1.14-2.68), p = 0.01。淋巴结状态也与较差的PFS相关,N3疾病患者的中位PFS为5.1个月,而N0-N2疾病患者的中位PFS为15.2个月,HR为2.09 (95% CI 1.28-3.41), p = 0.003。在多变量分析中,PTV≥350 cm3和N3累及仍与PFS显著相关。这两个变量都与早期和远期复发模式相关,PTV≥350 cm3与较差的生存率相关。结论:本研究确定PTV≥350 cm3和淋巴结受累是接受CRT和Durvalumab治疗的III期NSCLC患者临床预后较差的关键预测因素。350 cm3的PTV阈值为风险分层提供了一个实用的、临床适用的工具,可以指导加强治疗和监测,以改善高危患者的预后。
期刊介绍:
Thoracic Cancer aims to facilitate international collaboration and exchange of comprehensive and cutting-edge information on basic, translational, and applied clinical research in lung cancer, esophageal cancer, mediastinal cancer, breast cancer and other thoracic malignancies. Prevention, treatment and research relevant to Asia-Pacific is a focus area, but submissions from all regions are welcomed. The editors encourage contributions relevant to prevention, general thoracic surgery, medical oncology, radiology, radiation medicine, pathology, basic cancer research, as well as epidemiological and translational studies in thoracic cancer. Thoracic Cancer is the official publication of the Chinese Society of Lung Cancer, International Chinese Society of Thoracic Surgery and is endorsed by the Korean Association for the Study of Lung Cancer and the Hong Kong Cancer Therapy Society.
The Journal publishes a range of article types including: Editorials, Invited Reviews, Mini Reviews, Original Articles, Clinical Guidelines, Technological Notes, Imaging in thoracic cancer, Meeting Reports, Case Reports, Letters to the Editor, Commentaries, and Brief Reports.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


