One versus two: How much does it matter? A single-center retrospective study evaluating 1-day extracorporeal photopheresis schedule for treating patients with chronic lung allograft rejection.
{"title":"One versus two: How much does it matter? A single-center retrospective study evaluating 1-day extracorporeal photopheresis schedule for treating patients with chronic lung allograft rejection.","authors":"Claudia Del Fante, Valentina Vertui, Catherine Klersy, Cristina Mortellaro, Domenica Federica Briganti, Letizia Corinna Morlacchi, Marianna Russo, Cesare Perotti, Federica Meloni","doi":"10.1111/trf.18318","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Several studies show that extracorporeal photopheresis (ECP) might benefit chronic lung allograft dysfunction (CLAD). A standard ECP cycle consists of two consecutive procedures regardless of the technique employed.</p><p><strong>Study design and methods: </strong>Evaluation of ECP cycle (from two to one procedure) modification due to pandemic restrictions in 25 patients with CLAD under chronic treatment by off-line ECP in the 6 months preceding cycle modification (one procedure processing 1.5 patients blood volumes [1.5 ECP]). Assessment of any significant change in lung function decline and the relationship with product characteristics compared to pre-ECP cycle modification.</p><p><strong>Results: </strong>ECP patients (23 obstructive and two mixed) were enrolled in 2020 during the COVID pandemic. Two hundred and thirty five ECP procedures followed the standard protocol and 121 the 1.5 ECP. There was little or no variation in lung function during the study period. The mean number of mononuclear cells (MNC) per kg administered over time was higher in the 1.5 ECP than in the standard ECP protocol (p = .014). No association was found between respiratory function and MNC infused. Persistent Forced Expiratory Volume in 1 s decline >10% was observed in two patients over the 6 months preceding 1.5 ECP (due to CLAD progression) and in three patients after 1.5 ECP initiation (one for CLAD progression, two for bronchial colonization).</p><p><strong>Conclusion: </strong>Our study shows that respiratory function is maintained over time and is comparable between both ECP strategies in responders. The shift from two to one procedure per cycle may be reasonable in CLAD patients treated by off-line ECP.</p>","PeriodicalId":23266,"journal":{"name":"Transfusion","volume":" ","pages":"1490-1501"},"PeriodicalIF":2.0000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12315613/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Transfusion","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/trf.18318","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/14 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Several studies show that extracorporeal photopheresis (ECP) might benefit chronic lung allograft dysfunction (CLAD). A standard ECP cycle consists of two consecutive procedures regardless of the technique employed.
Study design and methods: Evaluation of ECP cycle (from two to one procedure) modification due to pandemic restrictions in 25 patients with CLAD under chronic treatment by off-line ECP in the 6 months preceding cycle modification (one procedure processing 1.5 patients blood volumes [1.5 ECP]). Assessment of any significant change in lung function decline and the relationship with product characteristics compared to pre-ECP cycle modification.
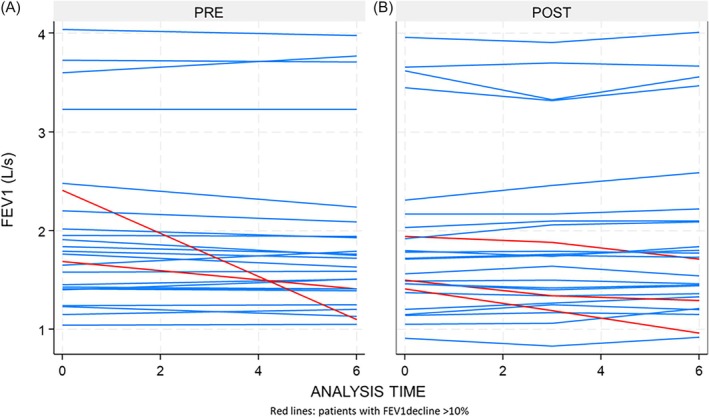
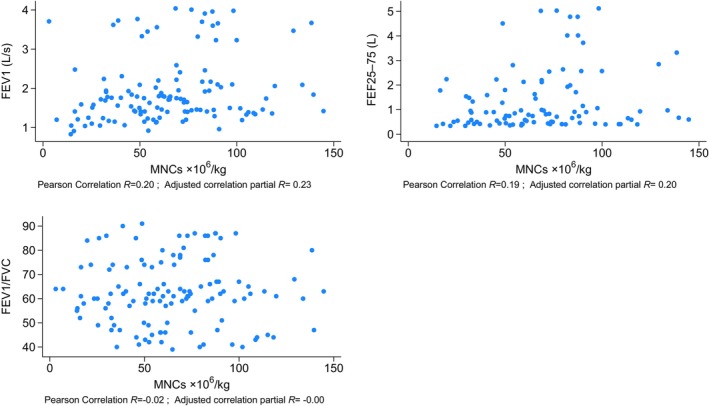
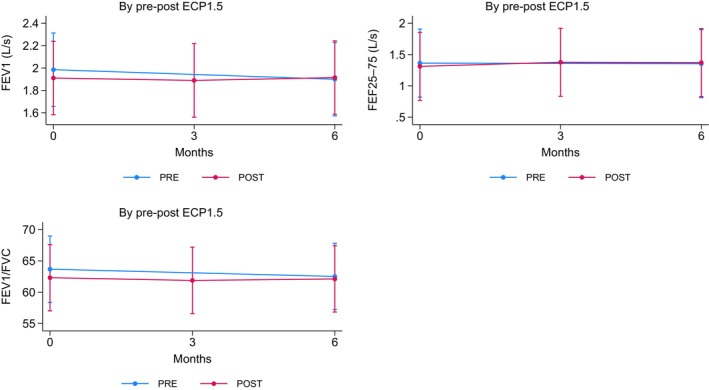
Results: ECP patients (23 obstructive and two mixed) were enrolled in 2020 during the COVID pandemic. Two hundred and thirty five ECP procedures followed the standard protocol and 121 the 1.5 ECP. There was little or no variation in lung function during the study period. The mean number of mononuclear cells (MNC) per kg administered over time was higher in the 1.5 ECP than in the standard ECP protocol (p = .014). No association was found between respiratory function and MNC infused. Persistent Forced Expiratory Volume in 1 s decline >10% was observed in two patients over the 6 months preceding 1.5 ECP (due to CLAD progression) and in three patients after 1.5 ECP initiation (one for CLAD progression, two for bronchial colonization).
Conclusion: Our study shows that respiratory function is maintained over time and is comparable between both ECP strategies in responders. The shift from two to one procedure per cycle may be reasonable in CLAD patients treated by off-line ECP.
期刊介绍:
TRANSFUSION is the foremost publication in the world for new information regarding transfusion medicine. Written by and for members of AABB and other health-care workers, TRANSFUSION reports on the latest technical advances, discusses opposing viewpoints regarding controversial issues, and presents key conference proceedings. In addition to blood banking and transfusion medicine topics, TRANSFUSION presents submissions concerning patient blood management, tissue transplantation and hematopoietic, cellular, and gene therapies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


