Marco Di Monaco, Carlotta Castiglioni, Francesca Bardesono, Marco A Minetto, Chiara Busso, Giuseppe Massazza
{"title":"Prevalent vertebral fractures and the diabetic bone paradox in women who sustain a hip fracture: a cross-sectional study.","authors":"Marco Di Monaco, Carlotta Castiglioni, Francesca Bardesono, Marco A Minetto, Chiara Busso, Giuseppe Massazza","doi":"10.23736/S1973-9087.25.08894-X","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Patients with type 2 diabetes mellitus (T2DM) have enhanced fracture risk despite high bone mineral density (BMD), a phenomenon known as the diabetic bone paradox. Consistently with the paradox, hip fractures occur at higher BMD in women with T2DM than in controls. However, no studies have addressed BMD in women with T2DM who have prevalent vertebral fractures at the time of their first hip fracture.</p><p><strong>Aim: </strong>The aim of this study was to test the hypothesis that BMD levels could be higher in the hip-fracture women with versus without T2DM in the absence but not in the presence of prevalent vertebral fractures.</p><p><strong>Design: </strong>This was a cross-sectional study.</p><p><strong>Setting: </strong>The research took place in a rehabilitation ward.</p><p><strong>Population: </strong>The study involved women who were undergoing inpatient rehabilitation following a subacute hip fracture.</p><p><strong>Methods: </strong>We investigated hip-fracture women with and without prevalent vertebral fractures, consecutively admitted to our rehabilitation ward. At a median of 19 days after the hip fracture we assessed femoral BMD by dual-energy X-ray absorptiometry and prevalent vertebral fractures by X-ray examination.</p><p><strong>Results: </strong>The study sample included 504 women. One hundred eighty-five of the 504 had no vertebral fractures whereas 319 had at least one spine fracture. The 185 women without vertebral fractures had BMD higher in the presence (N.=29) than in the absence (N.=156) of T2DM (mean T-score difference was 0.67, 95% confidence interval (CI) from 0.31 to 1.03, P<0.001). After adjustment for 8 potential confounders, the odds ratio to have densitometric osteoporosis for a woman without T2DM was 3.21 (95% CI from 1.10 to 9.33, P=0.032). On the contrary, in the 319 women with vertebral fractures T2DM was not associated with BMD.</p><p><strong>Conclusions: </strong>At the time of an original hip fracture, we found a BMD gap between women with and without T2DM in the absence but not in the presence of prevalent vertebral fractures.</p><p><strong>Clinical rehabilitation impact: </strong>Adjustments of fracture risk calculation in T2DM have been authoritatively suggested, because high BMD levels may falsely lead to risk underestimation. Our data suggests that no adjustments may be needed for the risk estimation in patients with prevalent vertebral fractures. Further data from longitudinal studies are needed to define the role of both prevalent vertebral fractures and BMD in fracture risk of patients with T2DM.</p>","PeriodicalId":12044,"journal":{"name":"European journal of physical and rehabilitation medicine","volume":" ","pages":"543-550"},"PeriodicalIF":3.4000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12409357/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European journal of physical and rehabilitation medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.23736/S1973-9087.25.08894-X","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/14 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"REHABILITATION","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Patients with type 2 diabetes mellitus (T2DM) have enhanced fracture risk despite high bone mineral density (BMD), a phenomenon known as the diabetic bone paradox. Consistently with the paradox, hip fractures occur at higher BMD in women with T2DM than in controls. However, no studies have addressed BMD in women with T2DM who have prevalent vertebral fractures at the time of their first hip fracture.
Aim: The aim of this study was to test the hypothesis that BMD levels could be higher in the hip-fracture women with versus without T2DM in the absence but not in the presence of prevalent vertebral fractures.
Design: This was a cross-sectional study.
Setting: The research took place in a rehabilitation ward.
Population: The study involved women who were undergoing inpatient rehabilitation following a subacute hip fracture.
Methods: We investigated hip-fracture women with and without prevalent vertebral fractures, consecutively admitted to our rehabilitation ward. At a median of 19 days after the hip fracture we assessed femoral BMD by dual-energy X-ray absorptiometry and prevalent vertebral fractures by X-ray examination.
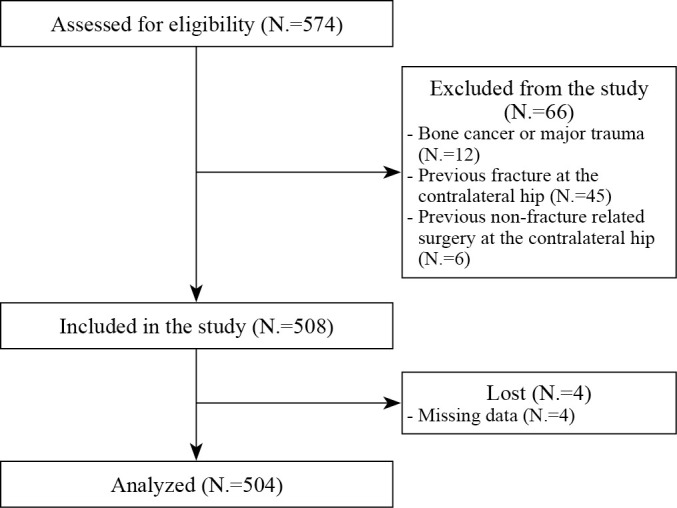
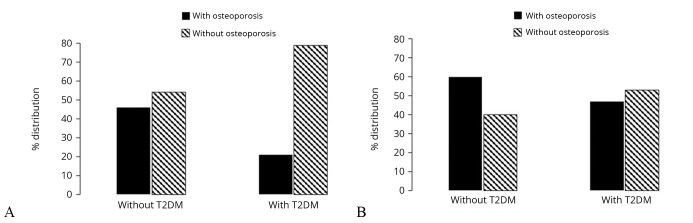
Results: The study sample included 504 women. One hundred eighty-five of the 504 had no vertebral fractures whereas 319 had at least one spine fracture. The 185 women without vertebral fractures had BMD higher in the presence (N.=29) than in the absence (N.=156) of T2DM (mean T-score difference was 0.67, 95% confidence interval (CI) from 0.31 to 1.03, P<0.001). After adjustment for 8 potential confounders, the odds ratio to have densitometric osteoporosis for a woman without T2DM was 3.21 (95% CI from 1.10 to 9.33, P=0.032). On the contrary, in the 319 women with vertebral fractures T2DM was not associated with BMD.
Conclusions: At the time of an original hip fracture, we found a BMD gap between women with and without T2DM in the absence but not in the presence of prevalent vertebral fractures.
Clinical rehabilitation impact: Adjustments of fracture risk calculation in T2DM have been authoritatively suggested, because high BMD levels may falsely lead to risk underestimation. Our data suggests that no adjustments may be needed for the risk estimation in patients with prevalent vertebral fractures. Further data from longitudinal studies are needed to define the role of both prevalent vertebral fractures and BMD in fracture risk of patients with T2DM.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


