MRI Enhancement Patterns After Resection of Sporadic Vestibular Schwannoma: Comparing Retrosigmoid and Translabyrinthine Approaches
Abstract
Objective
One theoretical disadvantage of the retrosigmoid approach is the inability to visualize tumor at the fundus of the internal auditory canal, potentially leading to a higher risk of residual tumor even when the surgeon reports a gross total resection. We sought to compare MRI enhancement patterns and their persistence following retrosigmoid and translabyrinthine vestibular schwannoma (VS) resection.
Methods
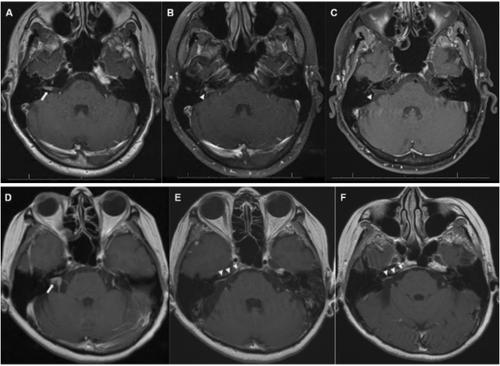
Adults aged ≥ 18 years old who underwent translabyrinthine or retrosigmoid approaches for resection of a sporadic vestibular schwannoma (VS) at a single tertiary care institution were eligible for inclusion in this cohort study. Patterns of enhancement on postoperative MRI, when present, were qualitatively described as linear or nodular. Multivariable logistic regression was used to adjust for tumor size and resection extent.
Results
After surgeon-reported gross total resection, linear enhancement was present in 24/141 (17.0%) and nodular enhancement in 2/141 (1.4%) cases. Both patterns showed high rates of spontaneous resolution, with 3/24 (12.5%) of linear enhancements persisting on ≥ 2 scans and no nodular enhancements (0/2) persisting. Among patients with less than gross total resection, when present, nodular enhancement was more likely to persist (3/5, 60.0%) than linear enhancement (3/8, 38.0%, p < 0.001). Approach was not associated with odds of nodular enhancement (OR for retrosigmoid vs. translabyrinthine 0.36, 95% Cl 0.05–1.89, p = 0.2). Similarly, surgical approach was not significantly associated with linear enhancement (p = 0.41). Surgeon-reported gross total resection was associated with reduced odds of nodular enhancement for translabyrinthine (OR 0.07, 95% CI 0.00–0.63, p = 0.04) but not retrosigmoid (OR 0.09, 95% CI 0.00–2.76, p = 0.13).
Conclusions
Postoperative enhancement typically resolves after gross total resection, but when present, surgeon-reported resection extent is a key predictor of persistence. However, our findings suggest that in retrosigmoid cases—where limited visualization of the fundus may increase the risk of residual tumor—surgeon reports of gross total resection may be less reliable.
Level of Evidence
IV.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


