Ahmed W Abbas, Mohamed F Abo-Elsoad, Mahmoud Diaa Hindawi, Mohamed Abo Zeid, Abd-Elfattah Kalmoush, Menna M Aboelkier, Mohamed A Aldemerdash, Rashad G Mohamed, Hosam Elghadban
{"title":"Prophylactic mesh reinforcement in elective abdominal surgeries: a systematic review, meta-analysis, and GRADE evidence assessment.","authors":"Ahmed W Abbas, Mohamed F Abo-Elsoad, Mahmoud Diaa Hindawi, Mohamed Abo Zeid, Abd-Elfattah Kalmoush, Menna M Aboelkier, Mohamed A Aldemerdash, Rashad G Mohamed, Hosam Elghadban","doi":"10.1007/s10029-025-03421-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Elective laparotomies account for a larger fraction of laparotomy procedures performed worldwide. Although surgical techniques continue to advance, the incidence of incisional hernia (IH) and other post-operative complications remain challenging to surgeons. This study aimed to evaluate the significance of using prophylactic mesh reinforcement during elective laparotomy.</p><p><strong>Methods: </strong>A comprehensive search was conducted in PubMed, Scopus, and Web of Science to identify studies that included adults undergoing elective abdominal surgery and compared prophylactic mesh reinforcement of the abdominal wall using any type of mesh in any anatomical position to standard fascial closure with sutures alone, without mesh. The analysis aimed to assess the impact of mesh reinforcement on the incidence of IH at all possible timepoints, in addition to secondary outcomes based on mesh technique, such as wound infections, dehiscence, seroma, re-operation for IH, and prolonged hospital stay. Data analysis was performed using the R programming language.</p><p><strong>Results: </strong>Fifteen RCTs, including 2,233 patients with follow-up durations ranging from 1.5 to 5 years, were analyzed. Prophylactic mesh reinforcement significantly reduced the incidence of IH following elective gastrointestinal surgeries at 12 months (risk ratio [RR] = 0.35, 95% confidence interval [CI] [0.14; 0.86], p = 0.02), 24 months (RR = 0.28, 95% CI [0.11; 0.68], p < 0.01), 36 months (RR = 0.62, 95% CI [0.36; 1.06], p = 0.08), and 48 months (RR = 0.35, 95% CI [0.11; 1.17], p = 0.09). Similarly, mesh significantly reduced IH rates following open abdominal aortic aneurysm repair at 12 months (RR = 0.13, 95% CI [0.04; 0.41], p < 0.01), 24 months (RR = 0.31, 95% CI [0.21; 0.45], p < 0.01), and 36 months (RR = 0.23, 95% CI [0.10; 0.54], p < 0.01).</p><p><strong>Conclusions: </strong>Prophylactic mesh reinforcement during elective abdominal laparotomy significantly reduced the incidence of IH and the need for reoperation. However, it is associated with an increased risk of seroma formation and, to a lesser extent, wound infection, particularly with the Sublay technique.</p>","PeriodicalId":13168,"journal":{"name":"Hernia","volume":"29 1","pages":"230"},"PeriodicalIF":2.4000,"publicationDate":"2025-07-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12254175/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Hernia","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10029-025-03421-9","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Elective laparotomies account for a larger fraction of laparotomy procedures performed worldwide. Although surgical techniques continue to advance, the incidence of incisional hernia (IH) and other post-operative complications remain challenging to surgeons. This study aimed to evaluate the significance of using prophylactic mesh reinforcement during elective laparotomy.
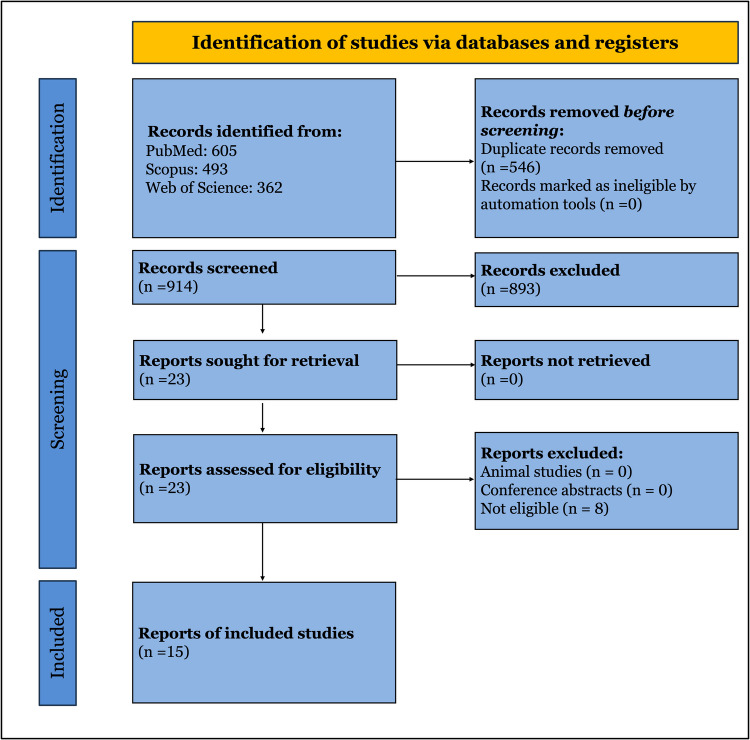
Methods: A comprehensive search was conducted in PubMed, Scopus, and Web of Science to identify studies that included adults undergoing elective abdominal surgery and compared prophylactic mesh reinforcement of the abdominal wall using any type of mesh in any anatomical position to standard fascial closure with sutures alone, without mesh. The analysis aimed to assess the impact of mesh reinforcement on the incidence of IH at all possible timepoints, in addition to secondary outcomes based on mesh technique, such as wound infections, dehiscence, seroma, re-operation for IH, and prolonged hospital stay. Data analysis was performed using the R programming language.
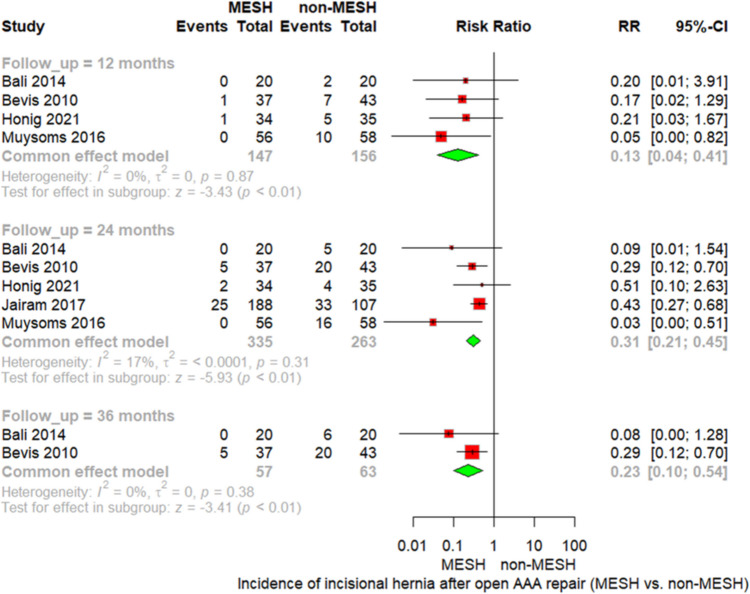
Results: Fifteen RCTs, including 2,233 patients with follow-up durations ranging from 1.5 to 5 years, were analyzed. Prophylactic mesh reinforcement significantly reduced the incidence of IH following elective gastrointestinal surgeries at 12 months (risk ratio [RR] = 0.35, 95% confidence interval [CI] [0.14; 0.86], p = 0.02), 24 months (RR = 0.28, 95% CI [0.11; 0.68], p < 0.01), 36 months (RR = 0.62, 95% CI [0.36; 1.06], p = 0.08), and 48 months (RR = 0.35, 95% CI [0.11; 1.17], p = 0.09). Similarly, mesh significantly reduced IH rates following open abdominal aortic aneurysm repair at 12 months (RR = 0.13, 95% CI [0.04; 0.41], p < 0.01), 24 months (RR = 0.31, 95% CI [0.21; 0.45], p < 0.01), and 36 months (RR = 0.23, 95% CI [0.10; 0.54], p < 0.01).
Conclusions: Prophylactic mesh reinforcement during elective abdominal laparotomy significantly reduced the incidence of IH and the need for reoperation. However, it is associated with an increased risk of seroma formation and, to a lesser extent, wound infection, particularly with the Sublay technique.
期刊介绍:
Hernia was founded in 1997 by Jean P. Chevrel with the purpose of promoting clinical studies and basic research as they apply to groin hernias and the abdominal wall . Since that time, a true revolution in the field of hernia studies has transformed the field from a ”simple” disease to one that is very specialized. While the majority of surgeries for primary inguinal and abdominal wall hernia are performed in hospitals worldwide, complex situations such as multi recurrences, complications, abdominal wall reconstructions and others are being studied and treated in specialist centers. As a result, major institutions and societies are creating specific parameters and criteria to better address the complexities of hernia surgery.
Hernia is a journal written by surgeons who have made abdominal wall surgery their specific field of interest, but we will consider publishing content from any surgeon who wishes to improve the science of this field. The Journal aims to ensure that hernia surgery is safer and easier for surgeons as well as patients, and provides a forum to all surgeons in the exchange of new ideas, results, and important research that is the basis of professional activity.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


