The role of intraabdominal drain placement in minimal-invasive right hemicolectomy with complete mesocolic excision - a propensity score matched single center analysis.
Maximilian Brunner, Katja Bondartschuk, Axel Denz, Georg F Weber, Robert Grützmann, Christian Krautz
{"title":"The role of intraabdominal drain placement in minimal-invasive right hemicolectomy with complete mesocolic excision - a propensity score matched single center analysis.","authors":"Maximilian Brunner, Katja Bondartschuk, Axel Denz, Georg F Weber, Robert Grützmann, Christian Krautz","doi":"10.1007/s00384-025-04948-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The role of intraabdominal drains in minimally invasive right hemicolectomy with complete mesocolic excision (CME) remains controversial. This study evaluates the impact of drain placement on perioperative outcomes using a propensity score-matched analysis in a single-center cohort.</p><p><strong>Methods: </strong>Data from 185 patients who underwent minimally invasive right hemicolectomy with complete mesocolic excision and central vascular ligation at our institution from 2016 to November 2024 were analyzed, including 62 without drains and 123 with drains. After propensity score matching, 50 patients from each group were compared. Postoperative outcomes were assessed between the groups and multivariate analysis was performed to identify risk factors for postoperative morbidity.</p><p><strong>Results: </strong>Postoperative complications, including morbidity (18% vs. 24%, p = 0.624), anastomotic leakage (2% vs. 2%, p = 1.000), surgical site infections (4% vs. 4%, p = 1.000) and re-surgery rate (2% vs. 6%, p = 0.617), did not differ significantly. However, the drain group showed delayed recovery milestones: longer time to first stool (2.1 vs. 2.7 days, p = 0.041), completion of meal plan (4.0 vs. 4.3 days, p = 0.038) and prolonged hospital stay (7 vs. 8 days, p = 0.045). Enhanced recovery rates were higher in the no-drain group (48% vs. 28%; p = 0.039). Multivariate analysis identified preoperative hemoglobin level ≤ 13 g/dl as a significant risk factor of postoperative complications (OR 9.8; 95% CI 2.0-48.7; p = 0.005), while drain placement was not significantly associated (p = 0.341).</p><p><strong>Conclusion: </strong>In minimally invasive right hemicolectomy with CME, routine drain placement does not reduce postoperative morbidity but may delay recovery milestones and prolong hospital stay. These findings suggest that selective rather than routine use of drains should be considered.</p>","PeriodicalId":13789,"journal":{"name":"International Journal of Colorectal Disease","volume":"40 1","pages":"156"},"PeriodicalIF":2.3000,"publicationDate":"2025-07-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12254058/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Colorectal Disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00384-025-04948-0","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The role of intraabdominal drains in minimally invasive right hemicolectomy with complete mesocolic excision (CME) remains controversial. This study evaluates the impact of drain placement on perioperative outcomes using a propensity score-matched analysis in a single-center cohort.
Methods: Data from 185 patients who underwent minimally invasive right hemicolectomy with complete mesocolic excision and central vascular ligation at our institution from 2016 to November 2024 were analyzed, including 62 without drains and 123 with drains. After propensity score matching, 50 patients from each group were compared. Postoperative outcomes were assessed between the groups and multivariate analysis was performed to identify risk factors for postoperative morbidity.
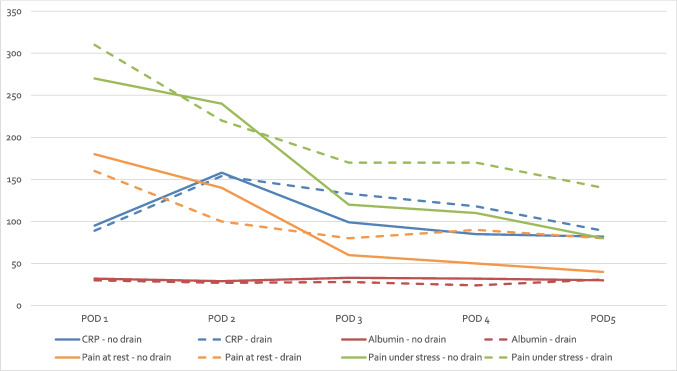
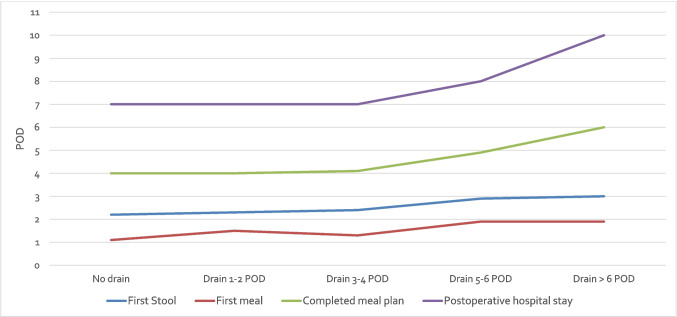
Results: Postoperative complications, including morbidity (18% vs. 24%, p = 0.624), anastomotic leakage (2% vs. 2%, p = 1.000), surgical site infections (4% vs. 4%, p = 1.000) and re-surgery rate (2% vs. 6%, p = 0.617), did not differ significantly. However, the drain group showed delayed recovery milestones: longer time to first stool (2.1 vs. 2.7 days, p = 0.041), completion of meal plan (4.0 vs. 4.3 days, p = 0.038) and prolonged hospital stay (7 vs. 8 days, p = 0.045). Enhanced recovery rates were higher in the no-drain group (48% vs. 28%; p = 0.039). Multivariate analysis identified preoperative hemoglobin level ≤ 13 g/dl as a significant risk factor of postoperative complications (OR 9.8; 95% CI 2.0-48.7; p = 0.005), while drain placement was not significantly associated (p = 0.341).
Conclusion: In minimally invasive right hemicolectomy with CME, routine drain placement does not reduce postoperative morbidity but may delay recovery milestones and prolong hospital stay. These findings suggest that selective rather than routine use of drains should be considered.
期刊介绍:
The International Journal of Colorectal Disease, Clinical and Molecular Gastroenterology and Surgery aims to publish novel and state-of-the-art papers which deal with the physiology and pathophysiology of diseases involving the entire gastrointestinal tract. In addition to original research articles, the following categories will be included: reviews (usually commissioned but may also be submitted), case reports, letters to the editor, and protocols on clinical studies.
The journal offers its readers an interdisciplinary forum for clinical science and molecular research related to gastrointestinal disease.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


