Optimization of vitamin K antagonist treatment: Near patient monitoring versus standard of care a parallel group clinical trial in older patients with atrial fibrillation.
Margriet van Elp, Maarten Beinema, Jacobus R B J Brouwers, Esther van 't Riet, Sjef van de Leur, Ildiko Schreiber, Frank G A Jansman
{"title":"Optimization of vitamin K antagonist treatment: Near patient monitoring versus standard of care a parallel group clinical trial in older patients with atrial fibrillation.","authors":"Margriet van Elp, Maarten Beinema, Jacobus R B J Brouwers, Esther van 't Riet, Sjef van de Leur, Ildiko Schreiber, Frank G A Jansman","doi":"10.1007/s00228-025-03878-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Atrial fibrillation (AF) is common in the elderly population and is associated with a high risk of thromboembolic events. Although non-vitamin K oral anticoagulants (NOACs) are the preferred drugs in antithrombotic therapy for AF, Vitamin K Anticoagulant drug (VKA) treatment is still used in a considerable proportion of patients with AF. Moreover, recent findings revealed that switching VKA to NOAC is associated with more bleeding complications in frail older patients with AF. Standard of care (SOC) monitoring of VKA treatment consists of venous blood sampling and back office dosage advice with a chain of processes and involvement of several health care professionals. We have designed a new procedure for monitoring (Near Patient Therapeutic Monitoring / NPTM) in order to improve the quality and safety of VKA treatment. NPTM consists of INR measurement with a point-of-care (POC) device in the home setting of a patient, performed by one professional and with an instant dosage advice.</p><p><strong>Methods: </strong>This is a cluster-randomised, parallel group, open label study to compare SOC with NPTM of VKA treatment in patients in a home setting. The follow-up period was one year. The primary outcome was time in therapeutic range (TTR), and secondary outcomes were adverse events (deaths, bleeding and thromboembolic events).</p><p><strong>Results: </strong>555 Patients were included in the study. After randomisation, 271 patients received SOC and 284 patients received NPTM. The TTR did not differ significantly: 63.71% versus 62.47% (p > 0.05) for SOC and NPTM, respectively. Significant differences were found for all-cause death (SOC n = 34 versus NPTM n = 16, p < 0.05, OR 0.47, 95% CI: 0.25-0.87), total number of minor bleedings (79 events in SOC vs 52 in NPTM, p < 0.05, OR 64 (95%CI: 0,37-0,81) and all non-major bleedings (100 events in SOC vs 67 in NPTM, p < 0.05, OR 0.62 (95% CI: 043-0.90).</p><p><strong>Conclusions: </strong>NPTM of VKA treatment in AF-patients does not result in an improved TTR when compared to SOC. All-cause death, total number of minor bleedings and all non-major bleedings may be reduced in NPTM, although the study was not powered for these secondary outcomes. Future studies are needed to determine the cost-effectiveness of NTPM versus SOC.</p>","PeriodicalId":11857,"journal":{"name":"European Journal of Clinical Pharmacology","volume":" ","pages":"1365-1371"},"PeriodicalIF":2.7000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12398432/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Clinical Pharmacology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00228-025-03878-8","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/12 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
Abstract
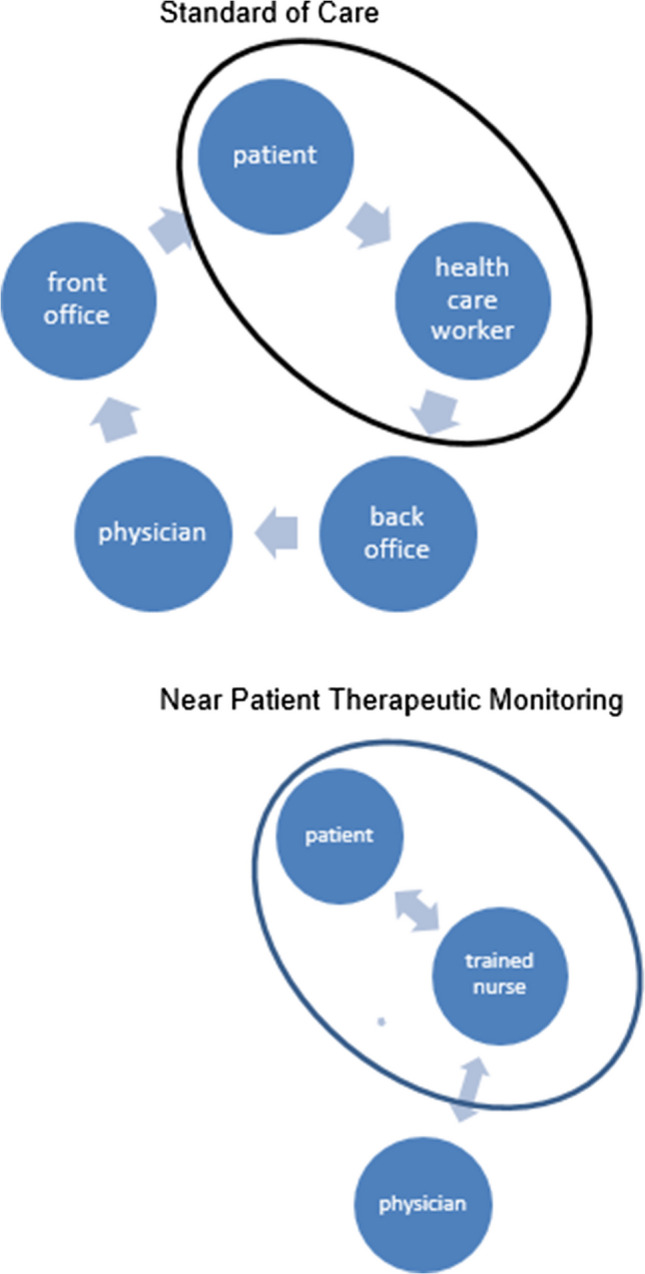
Purpose: Atrial fibrillation (AF) is common in the elderly population and is associated with a high risk of thromboembolic events. Although non-vitamin K oral anticoagulants (NOACs) are the preferred drugs in antithrombotic therapy for AF, Vitamin K Anticoagulant drug (VKA) treatment is still used in a considerable proportion of patients with AF. Moreover, recent findings revealed that switching VKA to NOAC is associated with more bleeding complications in frail older patients with AF. Standard of care (SOC) monitoring of VKA treatment consists of venous blood sampling and back office dosage advice with a chain of processes and involvement of several health care professionals. We have designed a new procedure for monitoring (Near Patient Therapeutic Monitoring / NPTM) in order to improve the quality and safety of VKA treatment. NPTM consists of INR measurement with a point-of-care (POC) device in the home setting of a patient, performed by one professional and with an instant dosage advice.
Methods: This is a cluster-randomised, parallel group, open label study to compare SOC with NPTM of VKA treatment in patients in a home setting. The follow-up period was one year. The primary outcome was time in therapeutic range (TTR), and secondary outcomes were adverse events (deaths, bleeding and thromboembolic events).
Results: 555 Patients were included in the study. After randomisation, 271 patients received SOC and 284 patients received NPTM. The TTR did not differ significantly: 63.71% versus 62.47% (p > 0.05) for SOC and NPTM, respectively. Significant differences were found for all-cause death (SOC n = 34 versus NPTM n = 16, p < 0.05, OR 0.47, 95% CI: 0.25-0.87), total number of minor bleedings (79 events in SOC vs 52 in NPTM, p < 0.05, OR 64 (95%CI: 0,37-0,81) and all non-major bleedings (100 events in SOC vs 67 in NPTM, p < 0.05, OR 0.62 (95% CI: 043-0.90).
Conclusions: NPTM of VKA treatment in AF-patients does not result in an improved TTR when compared to SOC. All-cause death, total number of minor bleedings and all non-major bleedings may be reduced in NPTM, although the study was not powered for these secondary outcomes. Future studies are needed to determine the cost-effectiveness of NTPM versus SOC.
期刊介绍:
The European Journal of Clinical Pharmacology publishes original papers on all aspects of clinical pharmacology and drug therapy in humans. Manuscripts are welcomed on the following topics: therapeutic trials, pharmacokinetics/pharmacodynamics, pharmacogenetics, drug metabolism, adverse drug reactions, drug interactions, all aspects of drug development, development relating to teaching in clinical pharmacology, pharmacoepidemiology, and matters relating to the rational prescribing and safe use of drugs. Methodological contributions relevant to these topics are also welcomed.
Data from animal experiments are accepted only in the context of original data in man reported in the same paper. EJCP will only consider manuscripts describing the frequency of allelic variants in different populations if this information is linked to functional data or new interesting variants. Highly relevant differences in frequency with a major impact in drug therapy for the respective population may be submitted as a letter to the editor.
Straightforward phase I pharmacokinetic or pharmacodynamic studies as parts of new drug development will only be considered for publication if the paper involves
-a compound that is interesting and new in some basic or fundamental way, or
-methods that are original in some basic sense, or
-a highly unexpected outcome, or
-conclusions that are scientifically novel in some basic or fundamental sense.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


