{"title":"Development and validation of a clinical prediction model for concurrent pulmonary infection in convalescent patients with intracerebral hemorrhage.","authors":"Jixiang Xu, Xiaoxiao Han, Yinliang Qi, Xiaomei Zhou","doi":"10.1186/s12938-025-01425-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>This study aimed to develop and validate a clinical prediction model for assessing the risk of concurrent pulmonary infection (PI) in patients recovering from intracerebral hemorrhage (ICH).</p><p><strong>Methods: </strong>In this retrospective study, we analyzed clinical data from 761 patients in the subacute recovery phase of ICH, of whom 504 developed PI and 257 did not. Univariate logistic regression was initially used to identify potential risk factors, followed by variable selection through the Least Absolute Shrinkage and Selection Operator (LASSO) regression. Predictors selected by LASSO were entered into a multivariate logistic regression to establish a final model. A nomogram was constructed based on the significant variables. The model's discrimination was evaluated using the area under the receiver operating characteristic curve (AUC), and its calibration was assessed using calibration plots and the Hosmer-Lemeshow goodness-of-fit test. Clinical utility was evaluated via decision curve analysis (DCA). Positive predictive value (PPV) and negative predictive value (NPV) were also calculated at the optimal threshold.</p><p><strong>Results: </strong>Eight independent predictors were identified: age, prophylactic antibiotic use, disturbance of consciousness, tracheotomy, dysphagia, duration of bed rest, nasal feeding, and procalcitonin level. The model demonstrated excellent discriminative ability with an AUC of 0.901(95%CI 0.878-0.924) and good calibration (Hosmer-Lemeshow test, P = 0.982). At the optimal cut-off point, the PPV was 92.6% and the NPV was 68.0%. DCA indicated favorable clinical benefit across a wide range of threshold probabilities.</p><p><strong>Conclusion: </strong>We developed a nomogram-based prediction model that accurately identifies the risk of pulmonary infection in patients recovering from ICH. This model offers valuable support for early clinical decision-making and targeted preventive strategies.</p>","PeriodicalId":8927,"journal":{"name":"BioMedical Engineering OnLine","volume":"24 1","pages":"88"},"PeriodicalIF":2.9000,"publicationDate":"2025-07-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12255977/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BioMedical Engineering OnLine","FirstCategoryId":"5","ListUrlMain":"https://doi.org/10.1186/s12938-025-01425-1","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ENGINEERING, BIOMEDICAL","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: This study aimed to develop and validate a clinical prediction model for assessing the risk of concurrent pulmonary infection (PI) in patients recovering from intracerebral hemorrhage (ICH).
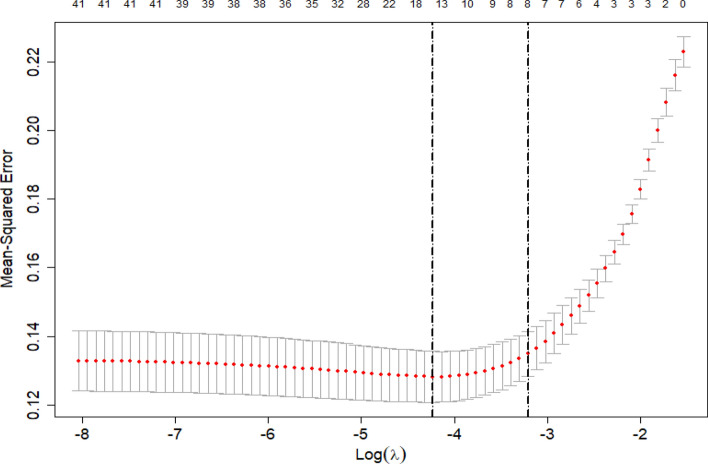
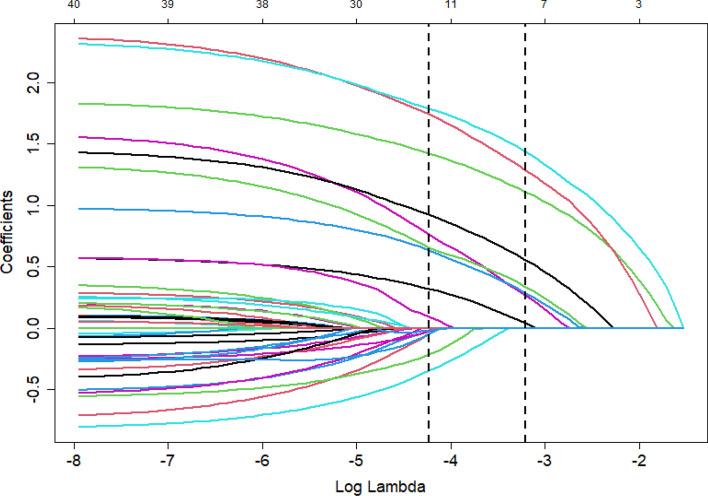
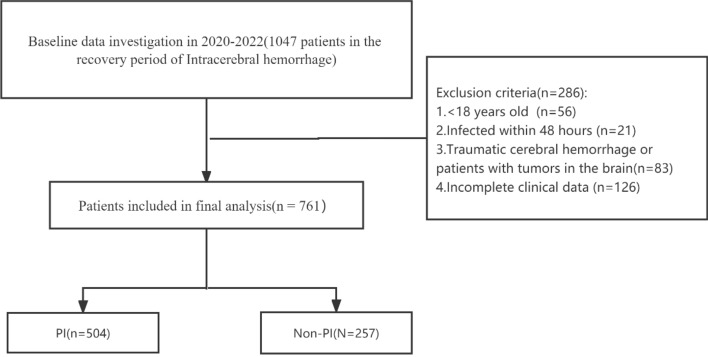
Methods: In this retrospective study, we analyzed clinical data from 761 patients in the subacute recovery phase of ICH, of whom 504 developed PI and 257 did not. Univariate logistic regression was initially used to identify potential risk factors, followed by variable selection through the Least Absolute Shrinkage and Selection Operator (LASSO) regression. Predictors selected by LASSO were entered into a multivariate logistic regression to establish a final model. A nomogram was constructed based on the significant variables. The model's discrimination was evaluated using the area under the receiver operating characteristic curve (AUC), and its calibration was assessed using calibration plots and the Hosmer-Lemeshow goodness-of-fit test. Clinical utility was evaluated via decision curve analysis (DCA). Positive predictive value (PPV) and negative predictive value (NPV) were also calculated at the optimal threshold.
Results: Eight independent predictors were identified: age, prophylactic antibiotic use, disturbance of consciousness, tracheotomy, dysphagia, duration of bed rest, nasal feeding, and procalcitonin level. The model demonstrated excellent discriminative ability with an AUC of 0.901(95%CI 0.878-0.924) and good calibration (Hosmer-Lemeshow test, P = 0.982). At the optimal cut-off point, the PPV was 92.6% and the NPV was 68.0%. DCA indicated favorable clinical benefit across a wide range of threshold probabilities.
Conclusion: We developed a nomogram-based prediction model that accurately identifies the risk of pulmonary infection in patients recovering from ICH. This model offers valuable support for early clinical decision-making and targeted preventive strategies.
期刊介绍:
BioMedical Engineering OnLine is an open access, peer-reviewed journal that is dedicated to publishing research in all areas of biomedical engineering.
BioMedical Engineering OnLine is aimed at readers and authors throughout the world, with an interest in using tools of the physical and data sciences and techniques in engineering to understand and solve problems in the biological and medical sciences. Topical areas include, but are not limited to:
Bioinformatics-
Bioinstrumentation-
Biomechanics-
Biomedical Devices & Instrumentation-
Biomedical Signal Processing-
Healthcare Information Systems-
Human Dynamics-
Neural Engineering-
Rehabilitation Engineering-
Biomaterials-
Biomedical Imaging & Image Processing-
BioMEMS and On-Chip Devices-
Bio-Micro/Nano Technologies-
Biomolecular Engineering-
Biosensors-
Cardiovascular Systems Engineering-
Cellular Engineering-
Clinical Engineering-
Computational Biology-
Drug Delivery Technologies-
Modeling Methodologies-
Nanomaterials and Nanotechnology in Biomedicine-
Respiratory Systems Engineering-
Robotics in Medicine-
Systems and Synthetic Biology-
Systems Biology-
Telemedicine/Smartphone Applications in Medicine-
Therapeutic Systems, Devices and Technologies-
Tissue Engineering

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


