Direct Oral Anticoagulants versus Aspirin for Secondary Stroke Prevention in Patients with Embolic Stroke of Undetermined Source: An Updated Systematic Review and Meta-Analysis of Randomized Controlled Trials.
Juan Armando Talavera, Larissa Teixeira, Thomas Costa Alexandre, Denilsa Navalha, Tathiane Brum Gibicoski, Nicole Fernandez, Jeffrey Healey, Luciana Armaganijan, Guilherme Dagostin de Carvalho
{"title":"Direct Oral Anticoagulants versus Aspirin for Secondary Stroke Prevention in Patients with Embolic Stroke of Undetermined Source: An Updated Systematic Review and Meta-Analysis of Randomized Controlled Trials.","authors":"Juan Armando Talavera, Larissa Teixeira, Thomas Costa Alexandre, Denilsa Navalha, Tathiane Brum Gibicoski, Nicole Fernandez, Jeffrey Healey, Luciana Armaganijan, Guilherme Dagostin de Carvalho","doi":"10.36660/abc.20240586","DOIUrl":null,"url":null,"abstract":"<p><p>Embolic stroke of undetermined source (ESUS) accounts for around 20% of ischemic strokes. The ideal treatment for secondary prevention in ESUS remains unclear. This study aimed to perform a systematic review and meta-analysis of randomized controlled trials (RCTs) comparing the safety and efficacy of direct oral anticoagulants (DOACs) versus aspirin in patients with ESUS. A systematic search of PubMed, Embase, Cochrane, and Web of Science databases was conducted for eligible trials until March 2024. The primary outcome was recurrent stroke, while safety outcomes included major bleeding and clinically relevant non-major bleeding (CRNMB). Hazard ratios (HRs) with 95% confidence intervals (CIs) were calculated for analysis. Four RCTs were included, involving 13,970 patients, half of whom were randomized to the DOACs group. Over a mean follow-up of 16 months, DOACs did not significantly reduce recurrent stroke (HR: 0.95; 95% CI: 0.81-1.09; p=0.44), ischemic stroke (HR: 0.91; 95% CI: 0.79-1.06; p=0.23), all-cause mortality (HR: 1.11; 95% CI: 0.87-1.42; p=0.40), or major bleeding (HR: 1.56; 95% CI: 0.85%-2.86; p=0.15) compared to aspirin. However, DOACs were associated with a significantly higher risk of CRNMB (HR: 1.54; 95% CI: 1.23-1.92; p=0.0002). Subgroup analysis revealed no significant differences in stroke recurrence among patients with low or high CHA2-DS2-VASc scores. DOACs did not demonstrate superior efficacy over aspirin in preventing recurrent stroke among ESUS patients and were linked to an increased risk of CRNMB.</p>","PeriodicalId":93887,"journal":{"name":"Arquivos brasileiros de cardiologia","volume":"122 6","pages":"e20240586"},"PeriodicalIF":1.9000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12269895/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Arquivos brasileiros de cardiologia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.36660/abc.20240586","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
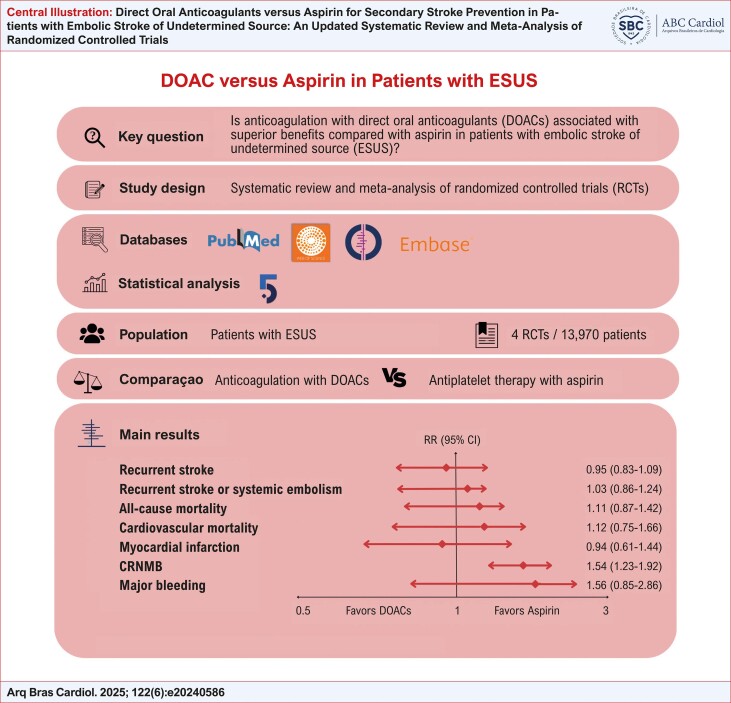
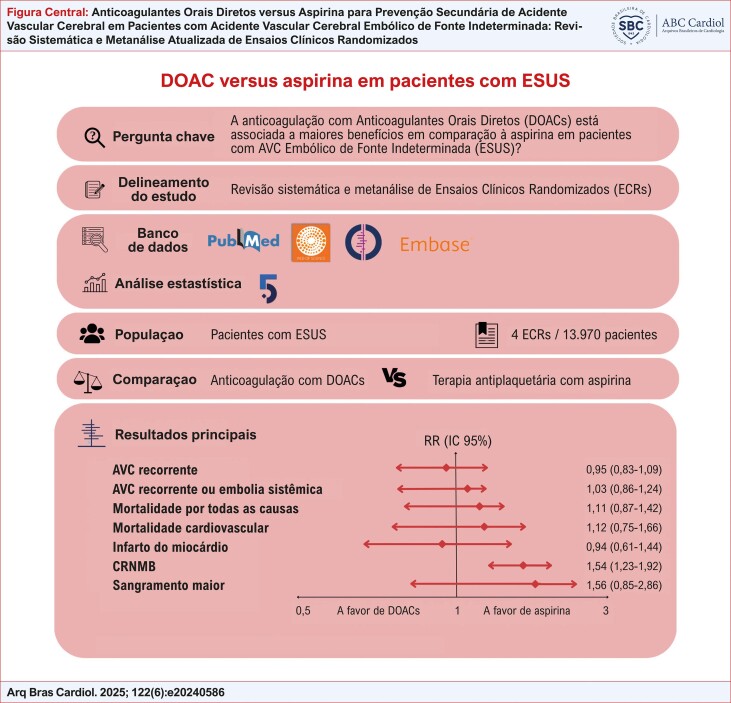
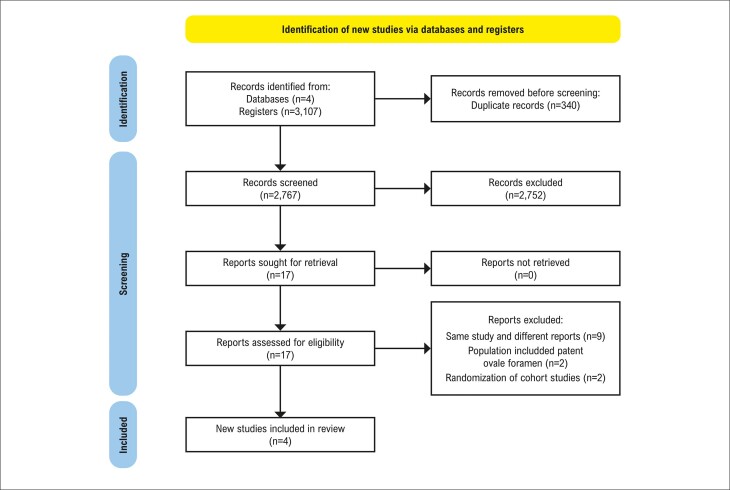
Embolic stroke of undetermined source (ESUS) accounts for around 20% of ischemic strokes. The ideal treatment for secondary prevention in ESUS remains unclear. This study aimed to perform a systematic review and meta-analysis of randomized controlled trials (RCTs) comparing the safety and efficacy of direct oral anticoagulants (DOACs) versus aspirin in patients with ESUS. A systematic search of PubMed, Embase, Cochrane, and Web of Science databases was conducted for eligible trials until March 2024. The primary outcome was recurrent stroke, while safety outcomes included major bleeding and clinically relevant non-major bleeding (CRNMB). Hazard ratios (HRs) with 95% confidence intervals (CIs) were calculated for analysis. Four RCTs were included, involving 13,970 patients, half of whom were randomized to the DOACs group. Over a mean follow-up of 16 months, DOACs did not significantly reduce recurrent stroke (HR: 0.95; 95% CI: 0.81-1.09; p=0.44), ischemic stroke (HR: 0.91; 95% CI: 0.79-1.06; p=0.23), all-cause mortality (HR: 1.11; 95% CI: 0.87-1.42; p=0.40), or major bleeding (HR: 1.56; 95% CI: 0.85%-2.86; p=0.15) compared to aspirin. However, DOACs were associated with a significantly higher risk of CRNMB (HR: 1.54; 95% CI: 1.23-1.92; p=0.0002). Subgroup analysis revealed no significant differences in stroke recurrence among patients with low or high CHA2-DS2-VASc scores. DOACs did not demonstrate superior efficacy over aspirin in preventing recurrent stroke among ESUS patients and were linked to an increased risk of CRNMB.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


