Irene López-Ferreruela, Antonio Gimeno-Miguel, Clara Laguna-Berna, Sara Malo, Sara Castel-Feced, María José Rabanaque, Isabel Aguilar-Palacio
{"title":"When gender matters: inequalities in health services utilization and risk factors monitoring after acute myocardial infarction.","authors":"Irene López-Ferreruela, Antonio Gimeno-Miguel, Clara Laguna-Berna, Sara Malo, Sara Castel-Feced, María José Rabanaque, Isabel Aguilar-Palacio","doi":"10.3389/fgwh.2025.1605400","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Secondary prevention after an acute myocardial infarction (AMI) has the objective of improving quality of life, minimizing recurrence, and reducing morbidity and mortality. Despite European guidelines highlighting the importance of cardiovascular risk factor (CVRF) management and optimal healthcare utilization, inequalities persist, particularly between genders. This study aims to identify and analyze gender inequalities in healthcare utilization and CVRF monitoring during the first year after AMI using real-world data (RWD).</p><p><strong>Methods: </strong>An analytical study was conducted within the CARhES (CArdiovascular Risk factors for Health Services research) cohort in Aragon, Spain. The study population included 3,464 subjects who survived a first AMI and were followed for one full year after the event. Sociodemographic, anthropometric, clinical data, healthcare utilization, CVRF monitoring and pharmacological prescriptions, were extracted from the Aragon Health Service. Statistical analyses included chi-squared tests, Student's <i>t</i>-tests, and logistic regression, with Blinder-Oaxaca decomposition applied to explore possible explanatory factors for gender differences.</p><p><strong>Results: </strong>Women represented 28.3% of the study population. Compared with men, they were older and had a higher morbidity burden. Primary care utilization was similar between genders; however, women had fewer cardiology visits (<i>p</i> < 0.001) and were less likely to achieve risk factor monitoring goals. Differences were also observed in pharmacological treatment, with women being less likely to receive beta-blockers, lipid modifying agents, and antiplatelet agents (<i>p</i> < 0.001). Several of these inequalities persisted after controlling for age. The Oaxaca decomposition showed that age and morbidity burden were the main contributors to gender disparities. In addition, socioeconomic status and place of residence played a role in health services utilization differences.</p><p><strong>Conclusions: </strong>Gender inequalities are still present in post-AMI care and CVRF management, with women being more likely to receive less adequate treatment and management. Addressing these inequalities is crucial to ensuring equitable care and improving health outcomes for women.</p>","PeriodicalId":73087,"journal":{"name":"Frontiers in global women's health","volume":"6 ","pages":"1605400"},"PeriodicalIF":2.4000,"publicationDate":"2025-06-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12241081/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in global women's health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3389/fgwh.2025.1605400","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Secondary prevention after an acute myocardial infarction (AMI) has the objective of improving quality of life, minimizing recurrence, and reducing morbidity and mortality. Despite European guidelines highlighting the importance of cardiovascular risk factor (CVRF) management and optimal healthcare utilization, inequalities persist, particularly between genders. This study aims to identify and analyze gender inequalities in healthcare utilization and CVRF monitoring during the first year after AMI using real-world data (RWD).
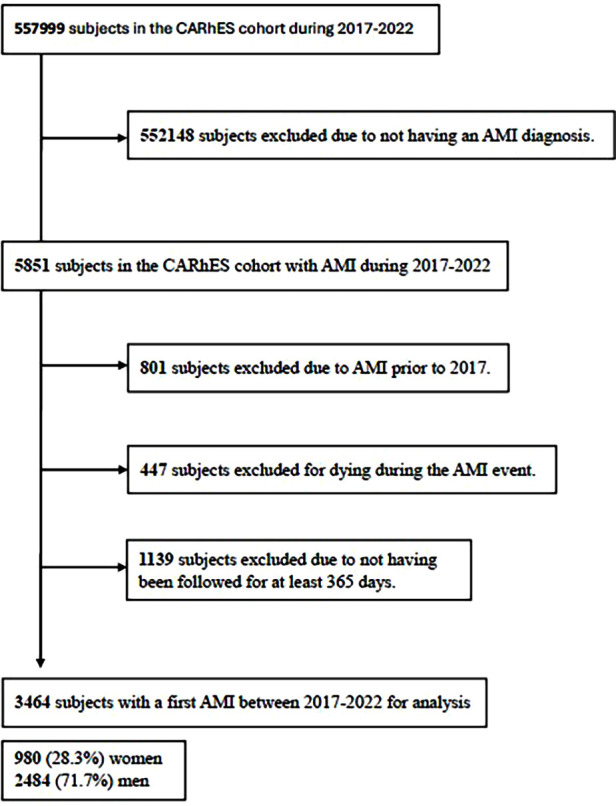
Methods: An analytical study was conducted within the CARhES (CArdiovascular Risk factors for Health Services research) cohort in Aragon, Spain. The study population included 3,464 subjects who survived a first AMI and were followed for one full year after the event. Sociodemographic, anthropometric, clinical data, healthcare utilization, CVRF monitoring and pharmacological prescriptions, were extracted from the Aragon Health Service. Statistical analyses included chi-squared tests, Student's t-tests, and logistic regression, with Blinder-Oaxaca decomposition applied to explore possible explanatory factors for gender differences.
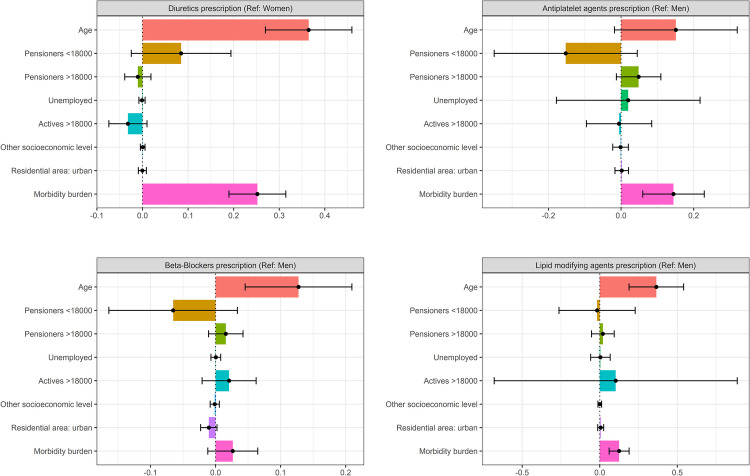
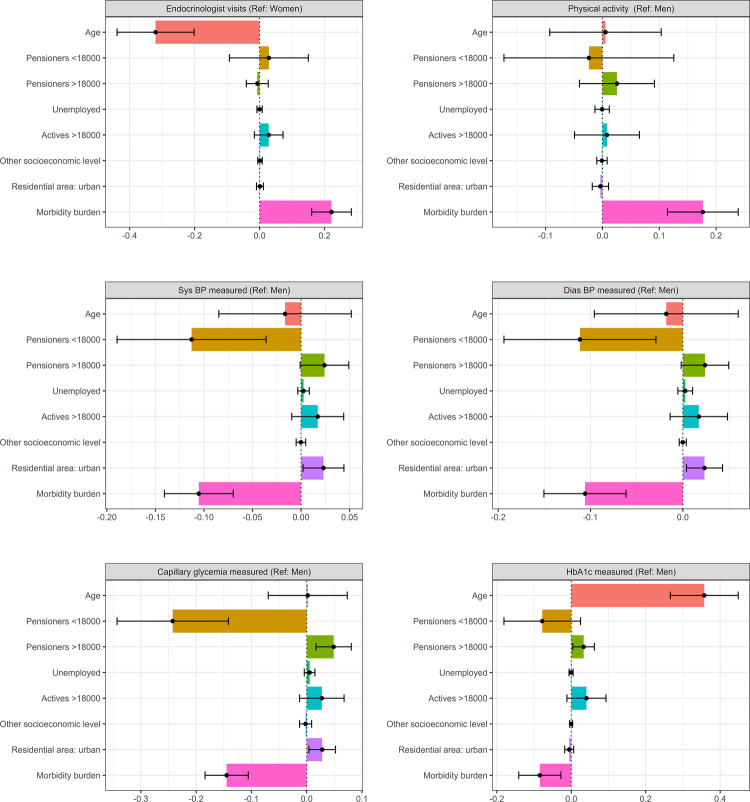
Results: Women represented 28.3% of the study population. Compared with men, they were older and had a higher morbidity burden. Primary care utilization was similar between genders; however, women had fewer cardiology visits (p < 0.001) and were less likely to achieve risk factor monitoring goals. Differences were also observed in pharmacological treatment, with women being less likely to receive beta-blockers, lipid modifying agents, and antiplatelet agents (p < 0.001). Several of these inequalities persisted after controlling for age. The Oaxaca decomposition showed that age and morbidity burden were the main contributors to gender disparities. In addition, socioeconomic status and place of residence played a role in health services utilization differences.
Conclusions: Gender inequalities are still present in post-AMI care and CVRF management, with women being more likely to receive less adequate treatment and management. Addressing these inequalities is crucial to ensuring equitable care and improving health outcomes for women.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


