Construction of a column-line graphical model of poor outcome of neoadjuvant regimens for muscle-invasive bladder cancer based on NLR, dNLR and SII indicators.
{"title":"Construction of a column-line graphical model of poor outcome of neoadjuvant regimens for muscle-invasive bladder cancer based on NLR, dNLR and SII indicators.","authors":"Bo Hu, Longsheng Wang, Shanna Qu, Tao Zhang","doi":"10.1186/s12957-025-03903-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>To study the effect and predict the value of neoadjuvant treatment regimen for muscle invasive bladder cancer (MIBC) by construction of a columnar graphical model of patients by neutrophil-to-lymphocyte ratio (NLR), derived neutrophil-to-lymphocyte ratio (dNLR), and systemic immune-inflammatory index (SII) indexes.</p><p><strong>Methods: </strong>265 patients with MIBC included from May 2022 to May 2024 were retrospectively selected to receive neoadjuvant treatment regimen respectively with treatment effect assessed, among which those achieving complete response (CR), partial response (PR), or stable disease (SD) were included in responders group and those with progressive disease (PD) in non-responders group. Clinical data of both groups were compared, related factors affecting the poor outcome after neoadjuvant therapy for MIBC were analyzed by Logistic regression, ensued with analysis of predictive value of poor prognosis by construction of a columnar graph model based on the NLR, dNLR and SII indexes.</p><p><strong>Results: </strong>A total of 265 patients with MIBC were included in this paper with a disease control rate (DCR) of 84.53% (224/265) after treatment with neoadjuvant regimen, among which 224 cases with controlled disease were involved in responders group and the remaining 41 cases with PD in non-responders group. Significant differences were observed between the two groups in terms of the degree of differentiation, tumor stage, NLR, dNLR and SII index levels (P < 0.05). After the diagnosis of covariance, the VIF values of the degree of differentiation and tumor stage were 5.535 and 5.582 respectively with a tolerance of 0.181 and 0.179, indicating that there existed a covariance problem (VIF value > 5) and could be moved out of the model followed by secondary analysis. Variables with P < 0.05 in the univariate factors were involved in the multivariate Logistic regression model with results showing that NLR, dNLR, and SII were all influential factors for the poor outcome of neoadjuvant regimens after treatment of MIBC (P < 0.05). Next, the column line graph, calibration curve and ROC curve graph were constructed. It was found that the AUC of the column line graph model in predicting poor outcome after neoadjuvant regimen for MIBC registered 0.995 (95% CI: 0.99-1.00), which was valuable in predicting poor outcome after neoadjuvant regimen for MIBC. CYFRA21-1, NMP22, and BTA were significantly higher in the poor response group than in the response group (P < 0.05), and CYFRA21-1, NMP22, and BTA showed a positive correlation with NLR, dNLR, and SII in both groups, respectively (P < 0.05).</p><p><strong>Conclusion: </strong>The neoadjuvant treatment program in patients with MIBC performed better, but some patients might still have a poor outcome with higher levels of NLR, dNLR and SII compared to those with a good outcome. In addition, the value of the combination of the three indicators in the prediction of the neoadjuvant treatment program displayed better performance, which was able to provide reference value for clinical decision-making.</p>","PeriodicalId":23856,"journal":{"name":"World Journal of Surgical Oncology","volume":"23 1","pages":"274"},"PeriodicalIF":2.5000,"publicationDate":"2025-07-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12247270/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Surgical Oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12957-025-03903-1","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: To study the effect and predict the value of neoadjuvant treatment regimen for muscle invasive bladder cancer (MIBC) by construction of a columnar graphical model of patients by neutrophil-to-lymphocyte ratio (NLR), derived neutrophil-to-lymphocyte ratio (dNLR), and systemic immune-inflammatory index (SII) indexes.
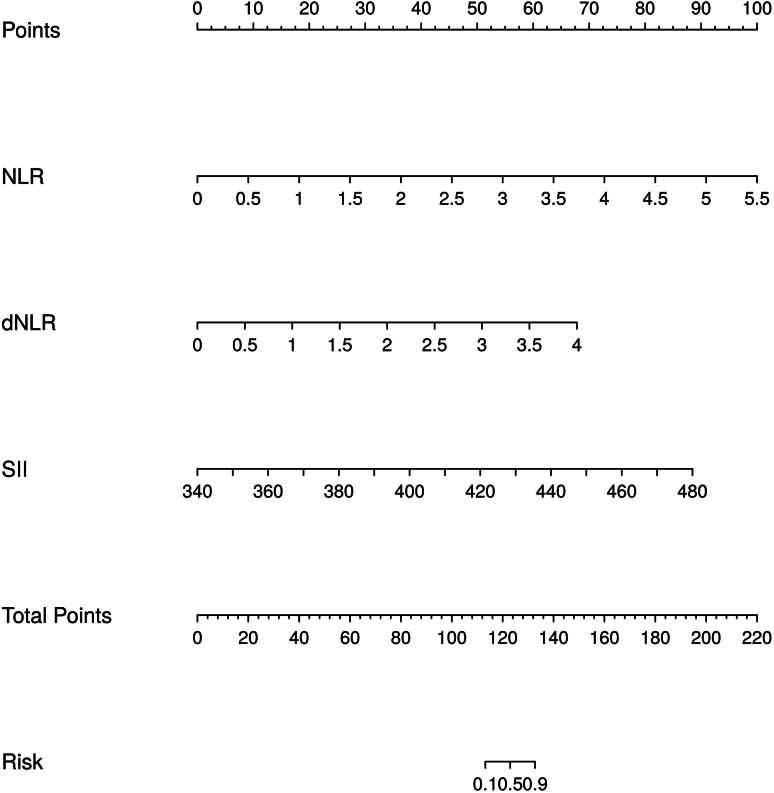
Methods: 265 patients with MIBC included from May 2022 to May 2024 were retrospectively selected to receive neoadjuvant treatment regimen respectively with treatment effect assessed, among which those achieving complete response (CR), partial response (PR), or stable disease (SD) were included in responders group and those with progressive disease (PD) in non-responders group. Clinical data of both groups were compared, related factors affecting the poor outcome after neoadjuvant therapy for MIBC were analyzed by Logistic regression, ensued with analysis of predictive value of poor prognosis by construction of a columnar graph model based on the NLR, dNLR and SII indexes.
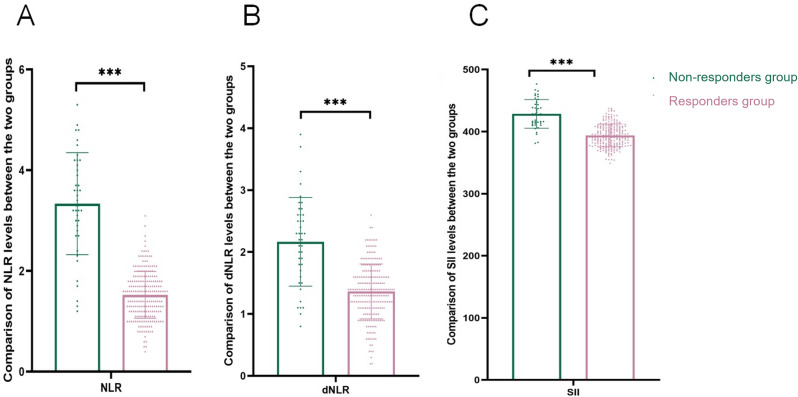
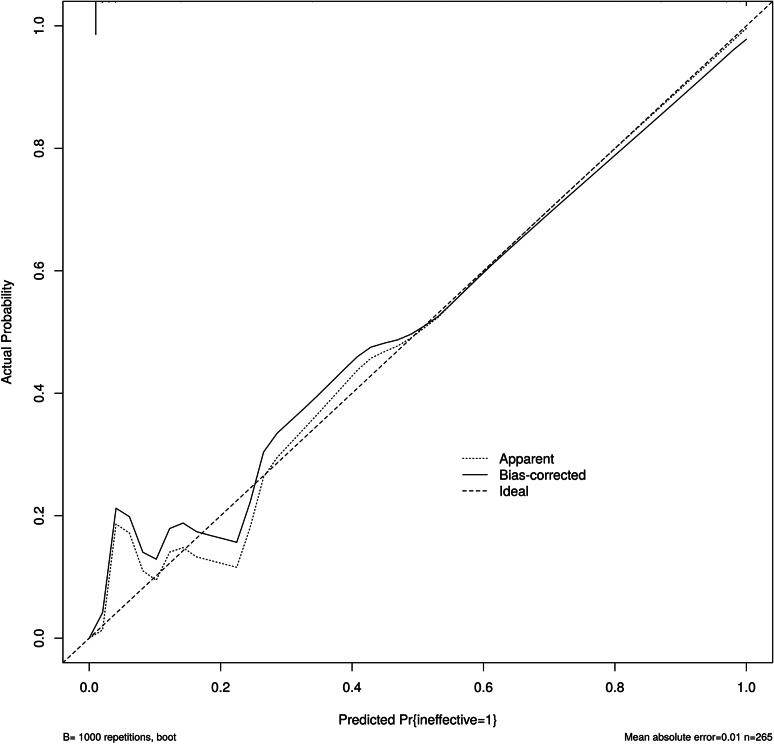
Results: A total of 265 patients with MIBC were included in this paper with a disease control rate (DCR) of 84.53% (224/265) after treatment with neoadjuvant regimen, among which 224 cases with controlled disease were involved in responders group and the remaining 41 cases with PD in non-responders group. Significant differences were observed between the two groups in terms of the degree of differentiation, tumor stage, NLR, dNLR and SII index levels (P < 0.05). After the diagnosis of covariance, the VIF values of the degree of differentiation and tumor stage were 5.535 and 5.582 respectively with a tolerance of 0.181 and 0.179, indicating that there existed a covariance problem (VIF value > 5) and could be moved out of the model followed by secondary analysis. Variables with P < 0.05 in the univariate factors were involved in the multivariate Logistic regression model with results showing that NLR, dNLR, and SII were all influential factors for the poor outcome of neoadjuvant regimens after treatment of MIBC (P < 0.05). Next, the column line graph, calibration curve and ROC curve graph were constructed. It was found that the AUC of the column line graph model in predicting poor outcome after neoadjuvant regimen for MIBC registered 0.995 (95% CI: 0.99-1.00), which was valuable in predicting poor outcome after neoadjuvant regimen for MIBC. CYFRA21-1, NMP22, and BTA were significantly higher in the poor response group than in the response group (P < 0.05), and CYFRA21-1, NMP22, and BTA showed a positive correlation with NLR, dNLR, and SII in both groups, respectively (P < 0.05).
Conclusion: The neoadjuvant treatment program in patients with MIBC performed better, but some patients might still have a poor outcome with higher levels of NLR, dNLR and SII compared to those with a good outcome. In addition, the value of the combination of the three indicators in the prediction of the neoadjuvant treatment program displayed better performance, which was able to provide reference value for clinical decision-making.
期刊介绍:
World Journal of Surgical Oncology publishes articles related to surgical oncology and its allied subjects, such as epidemiology, cancer research, biomarkers, prevention, pathology, radiology, cancer treatment, clinical trials, multimodality treatment and molecular biology. Emphasis is placed on original research articles. The journal also publishes significant clinical case reports, as well as balanced and timely reviews on selected topics.
Oncology is a multidisciplinary super-speciality of which surgical oncology forms an integral component, especially with solid tumors. Surgical oncologists around the world are involved in research extending from detecting the mechanisms underlying the causation of cancer, to its treatment and prevention. The role of a surgical oncologist extends across the whole continuum of care. With continued developments in diagnosis and treatment, the role of a surgical oncologist is ever-changing. Hence, World Journal of Surgical Oncology aims to keep readers abreast with latest developments that will ultimately influence the work of surgical oncologists.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


