The role of thymectomy during parathyroidectomy in multiple endocrine neoplasia type 1-associated hyperparathyroidism: a systematic review and meta-analysis.
Eman A Toraih, Mahmoud A AbdAlnaeem, Tanvi Bobba, Rami M Elshazli, Ahmed Abdelmaksoud, Yaser Y Bashumeel, Abdulrahman N Ghaleb, Mohammad H Hussein, Jessan A Jishu, Salem I Noureldine, Emad Kandil
{"title":"The role of thymectomy during parathyroidectomy in multiple endocrine neoplasia type 1-associated hyperparathyroidism: a systematic review and meta-analysis.","authors":"Eman A Toraih, Mahmoud A AbdAlnaeem, Tanvi Bobba, Rami M Elshazli, Ahmed Abdelmaksoud, Yaser Y Bashumeel, Abdulrahman N Ghaleb, Mohammad H Hussein, Jessan A Jishu, Salem I Noureldine, Emad Kandil","doi":"10.1186/s12957-025-03773-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Current guidelines recommend transcervical thymectomy (TCT) during parathyroidectomy (PTX) for Multiple Endocrine Neoplasia Type 1 (MEN1)-associated primary hyperparathyroidism (PHPT) despite limited evidence substantiating efficacy. We aimed to determine the role of TCT in disease control and safety outcomes.</p><p><strong>Methods: </strong>A systematic review and meta-analysis were conducted on comparative observational studies exploring the efficacy of PTX with or without concomitant TCT for managing PHPT in patients with MEN1. Pooled event proportions were estimated using Freeman-Tukey double arcsine transformation method and converted to relative risk. Six studies (n = 306 patients) were included.</p><p><strong>Results: </strong>TCT showed significantly reduced rates of persistent (relative risk 0.15; 21.9% vs. 3.1%; p < 0.01) and recurrent PHPT (RR 0.34, 43.8% vs. 12.9%; p = 0.004) necessitating re-operation compared to PTX alone, suggesting improved disease control. Interestingly, the addition of TCT reduced rates of transient PHPT (RR 0.07; 9.3% vs. 0%; p < 0.01 and permanent recurrent laryngeal nerve injury (RR 0.32, 3.9% vs. 1.0%; p = 0.04), indicating possible benefits in morbidity.</p><p><strong>Conclusions: </strong>Concomitant TCT may improve the safety and efficacy of PTX in MEN1-associated PHPT by synergistically clearing all cervical disease and minimizing adverse sequelae. Our findings provide further evidence to support existing recommendations for TCT and can guide surgical decision-making.</p>","PeriodicalId":23856,"journal":{"name":"World Journal of Surgical Oncology","volume":"23 1","pages":"272"},"PeriodicalIF":2.5000,"publicationDate":"2025-07-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12243190/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Surgical Oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12957-025-03773-7","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Current guidelines recommend transcervical thymectomy (TCT) during parathyroidectomy (PTX) for Multiple Endocrine Neoplasia Type 1 (MEN1)-associated primary hyperparathyroidism (PHPT) despite limited evidence substantiating efficacy. We aimed to determine the role of TCT in disease control and safety outcomes.
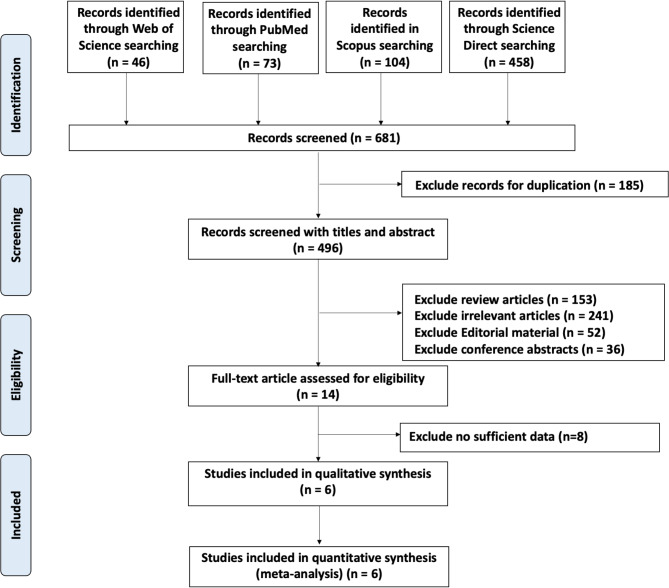
Methods: A systematic review and meta-analysis were conducted on comparative observational studies exploring the efficacy of PTX with or without concomitant TCT for managing PHPT in patients with MEN1. Pooled event proportions were estimated using Freeman-Tukey double arcsine transformation method and converted to relative risk. Six studies (n = 306 patients) were included.
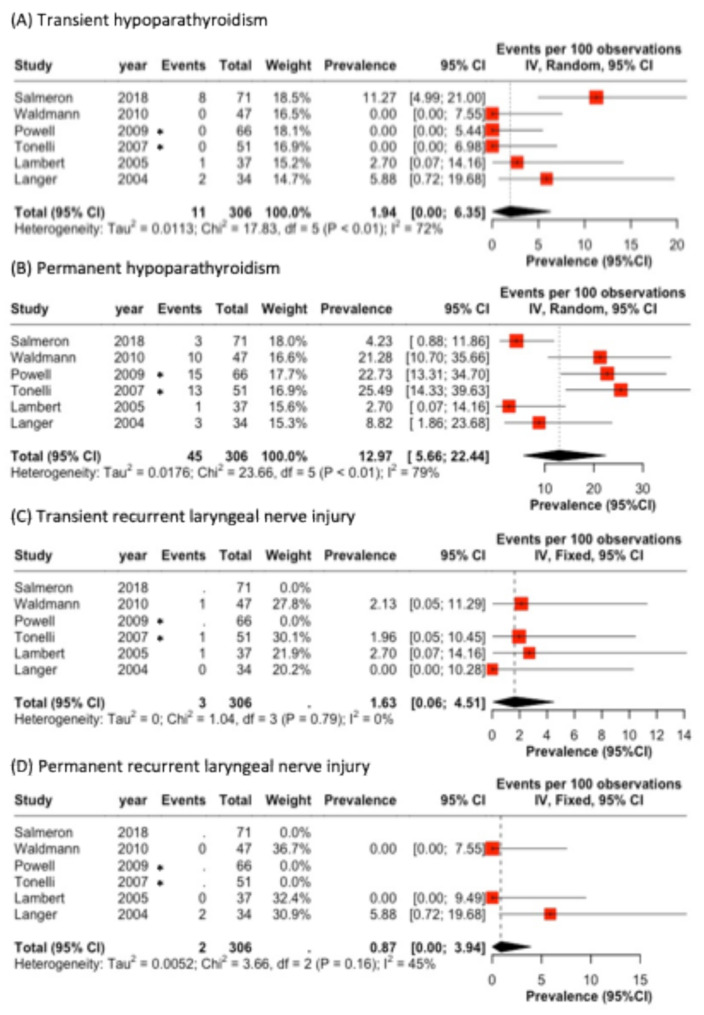
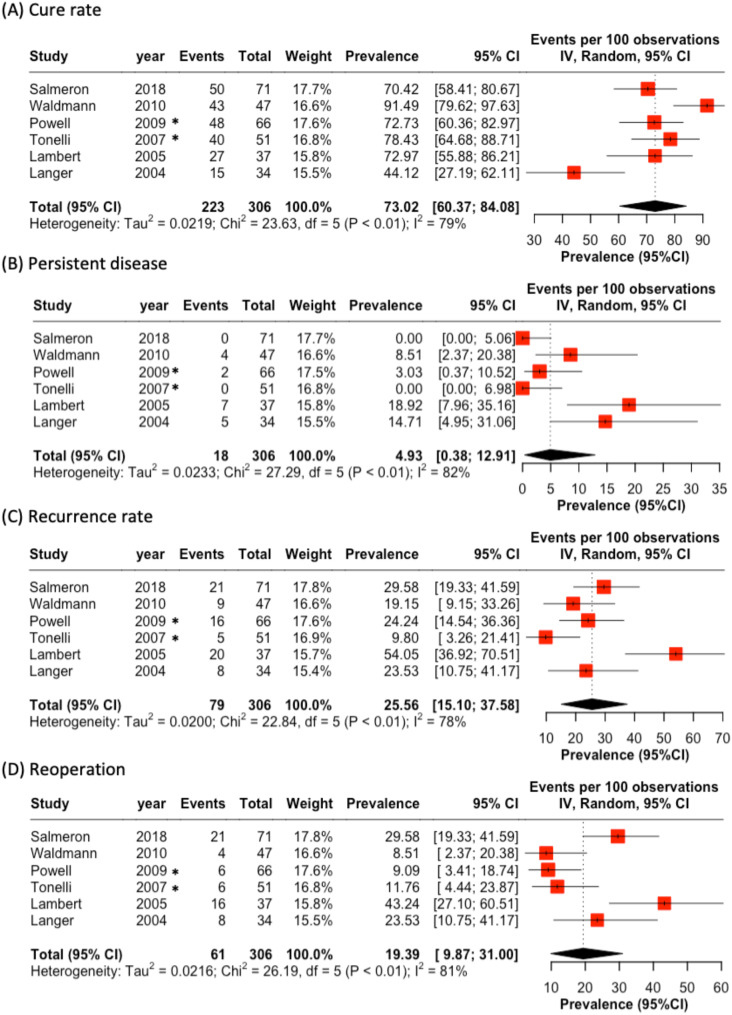
Results: TCT showed significantly reduced rates of persistent (relative risk 0.15; 21.9% vs. 3.1%; p < 0.01) and recurrent PHPT (RR 0.34, 43.8% vs. 12.9%; p = 0.004) necessitating re-operation compared to PTX alone, suggesting improved disease control. Interestingly, the addition of TCT reduced rates of transient PHPT (RR 0.07; 9.3% vs. 0%; p < 0.01 and permanent recurrent laryngeal nerve injury (RR 0.32, 3.9% vs. 1.0%; p = 0.04), indicating possible benefits in morbidity.
Conclusions: Concomitant TCT may improve the safety and efficacy of PTX in MEN1-associated PHPT by synergistically clearing all cervical disease and minimizing adverse sequelae. Our findings provide further evidence to support existing recommendations for TCT and can guide surgical decision-making.
背景:目前的指南建议在甲状旁腺切除术(PTX)期间进行经颈胸腺切除术(TCT)治疗多发性内分泌瘤1型(MEN1)相关的原发性甲状旁腺功能亢进(PHPT),尽管证据有限。我们的目的是确定TCT在疾病控制和安全性结果中的作用。方法:对比较观察性研究进行系统回顾和荟萃分析,探讨PTX合并或不合并TCT治疗MEN1患者PHPT的疗效。用Freeman-Tukey双反正弦变换法估计合并事件比例,并转换为相对风险。纳入6项研究(n = 306例患者)。结果:TCT显着降低了持续性(相对危险度0.15;21.9% vs. 3.1%;结论:合并TCT可通过协同清除所有宫颈疾病和减少不良后遗症,提高PTX治疗men1相关PHPT的安全性和有效性。我们的发现为现有的TCT建议提供了进一步的证据,并可以指导手术决策。
期刊介绍:
World Journal of Surgical Oncology publishes articles related to surgical oncology and its allied subjects, such as epidemiology, cancer research, biomarkers, prevention, pathology, radiology, cancer treatment, clinical trials, multimodality treatment and molecular biology. Emphasis is placed on original research articles. The journal also publishes significant clinical case reports, as well as balanced and timely reviews on selected topics.
Oncology is a multidisciplinary super-speciality of which surgical oncology forms an integral component, especially with solid tumors. Surgical oncologists around the world are involved in research extending from detecting the mechanisms underlying the causation of cancer, to its treatment and prevention. The role of a surgical oncologist extends across the whole continuum of care. With continued developments in diagnosis and treatment, the role of a surgical oncologist is ever-changing. Hence, World Journal of Surgical Oncology aims to keep readers abreast with latest developments that will ultimately influence the work of surgical oncologists.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


