Correlation of end-tidal carbon dioxide with transthoracic echocardiography derived cardiac output for the assessment of fluid responsiveness: A prospective observational study.
S Keerthi Raj, Debendra K Tripathy, Praveen Talawar, Deepak Singla
{"title":"Correlation of end-tidal carbon dioxide with transthoracic echocardiography derived cardiac output for the assessment of fluid responsiveness: A prospective observational study.","authors":"S Keerthi Raj, Debendra K Tripathy, Praveen Talawar, Deepak Singla","doi":"10.4103/joacp.joacp_288_24","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and aims: </strong>Judicious use of intravenous fluid therapy can be lifesaving in the intraoperative period. An assessment of fluid responsiveness is important for it. So, our study aimed to study the correlation between end-tidal carbon dioxide (EtCO<sub>2</sub>) and transthoracic echocardiography-derived cardiac output for assessing fluid responsiveness in patients undergoing elective surgery under general anesthesia.</p><p><strong>Material and methods: </strong>Patients who underwent elective lower abdominal or lower limb surgeries in a supine position under general anesthesia with positive pressure ventilation were included in this study. Cardiac output was calculated using transthoracic echo, and by measuring the diameter of the left ventricular outflow tract (LVOT), velocity time integral of LVOT (LVOT-VTI), and heart rate. Cardiac output (CO), EtCO<sub>2</sub>, and hemodynamic and ventilatory parameters were analyzed by the operator before and 1 min after the infusion of 250 mL of normal saline.</p><p><strong>Results: </strong>EtCO<sub>2</sub> variations showed a weak correlation with the changes in CO induced by a fluid challenge (Spearman's correlation <i>r =</i> 0.3, <i>P</i> = 0.005). When fluid responsiveness (FR) is defined as an increase in CO by > 15%, the AUROC of ∆ EtCO<sub>2</sub> was 0.638 (95% confidence interval [CI], 0.507-0.77). At a cut-off of ≥ 1 mmHg, it predicted FR status (responder vs. non-responder) with a sensitivity of 66% and a specificity of 64%. When percentage variation in EtCO<sub>2</sub> (percent ∆ EtCO<sub>2</sub>) was considered, the AUROC was almost similar (0.618) (95% CI, 0.481-0.756), and it was not statistically significant (<i>P</i> = 0.093).</p><p><strong>Conclusions: </strong>Our study demonstrated a weak positive correlation between volume-induced changes in EtCO<sub>2</sub> and changes in CO in mechanically ventilated patients in the operating room. Variations in EtCO<sub>2</sub> can be used as an adjunct to guide hemodynamic optimization when no COcardiac output monitors are available.</p>","PeriodicalId":14946,"journal":{"name":"Journal of Anaesthesiology, Clinical Pharmacology","volume":"41 3","pages":"478-485"},"PeriodicalIF":1.1000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12237246/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Anaesthesiology, Clinical Pharmacology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/joacp.joacp_288_24","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/19 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
Abstract
Background and aims: Judicious use of intravenous fluid therapy can be lifesaving in the intraoperative period. An assessment of fluid responsiveness is important for it. So, our study aimed to study the correlation between end-tidal carbon dioxide (EtCO2) and transthoracic echocardiography-derived cardiac output for assessing fluid responsiveness in patients undergoing elective surgery under general anesthesia.
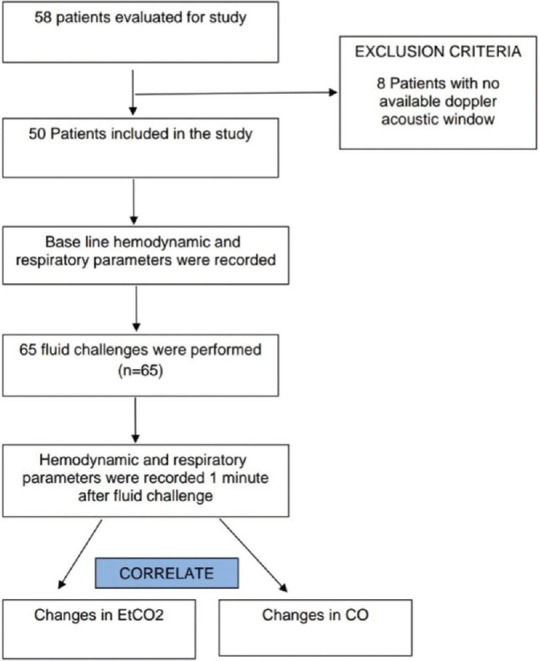
Material and methods: Patients who underwent elective lower abdominal or lower limb surgeries in a supine position under general anesthesia with positive pressure ventilation were included in this study. Cardiac output was calculated using transthoracic echo, and by measuring the diameter of the left ventricular outflow tract (LVOT), velocity time integral of LVOT (LVOT-VTI), and heart rate. Cardiac output (CO), EtCO2, and hemodynamic and ventilatory parameters were analyzed by the operator before and 1 min after the infusion of 250 mL of normal saline.
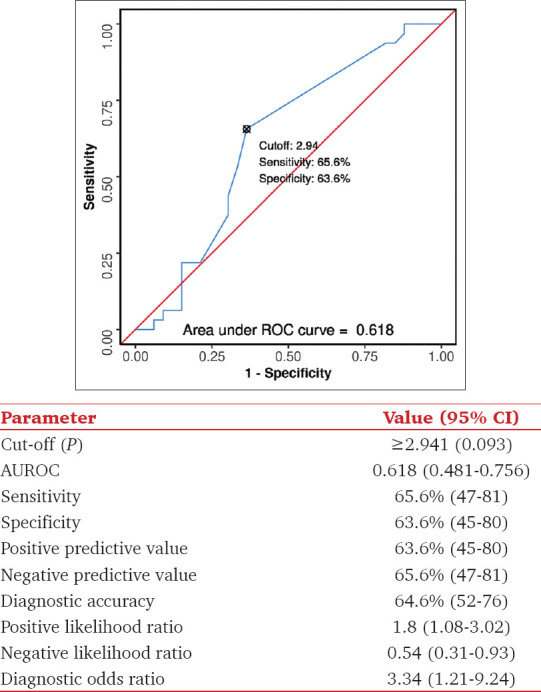
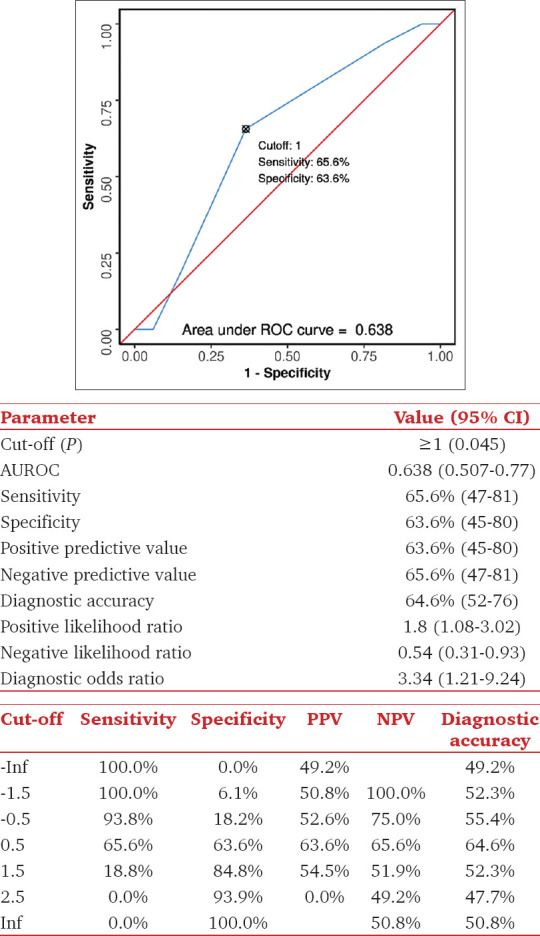
Results: EtCO2 variations showed a weak correlation with the changes in CO induced by a fluid challenge (Spearman's correlation r = 0.3, P = 0.005). When fluid responsiveness (FR) is defined as an increase in CO by > 15%, the AUROC of ∆ EtCO2 was 0.638 (95% confidence interval [CI], 0.507-0.77). At a cut-off of ≥ 1 mmHg, it predicted FR status (responder vs. non-responder) with a sensitivity of 66% and a specificity of 64%. When percentage variation in EtCO2 (percent ∆ EtCO2) was considered, the AUROC was almost similar (0.618) (95% CI, 0.481-0.756), and it was not statistically significant (P = 0.093).
Conclusions: Our study demonstrated a weak positive correlation between volume-induced changes in EtCO2 and changes in CO in mechanically ventilated patients in the operating room. Variations in EtCO2 can be used as an adjunct to guide hemodynamic optimization when no COcardiac output monitors are available.
期刊介绍:
The JOACP publishes original peer-reviewed research and clinical work in all branches of anaesthesiology, pain, critical care and perioperative medicine including the application to basic sciences. In addition, the journal publishes review articles, special articles, brief communications/reports, case reports, and reports of new equipment, letters to editor, book reviews and obituaries. It is international in scope and comprehensive in coverage.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


