Paula Rodríguez Payá, Álvaro Muñoz Abad, Beatriz Grau Mirete, Asia Ferrández Arias, Miguel Borregón Rivilla, Javier David Benítez Fuentes, Federico J Vázquez Mazón
{"title":"Successful Management of Immune-Mediated Myelitis in a Renal Cancer Patient: A Case Report.","authors":"Paula Rodríguez Payá, Álvaro Muñoz Abad, Beatriz Grau Mirete, Asia Ferrández Arias, Miguel Borregón Rivilla, Javier David Benítez Fuentes, Federico J Vázquez Mazón","doi":"10.1159/000543929","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Immune checkpoint inhibitors (ICIs) have revolutionized metastatic renal cell carcinoma treatment, significantly improving survival outcomes. However, ICIs are linked to immune-related adverse events (irAEs), which can impact multiple organs. Neurological irAEs, such as myelitis, are rare but potentially severe.</p><p><strong>Case presentation: </strong>We describe a 54-year-old male with high-grade clear cell renal carcinoma treated with nivolumab and ipilimumab. After four cycles, he developed hypophysitis, adrenal insufficiency, and hypothyroidism, managed with hydrocortisone and levothyroxine, while continuing nivolumab monotherapy. In August 2022, he experienced right eyelid ptosis and right hand weakness. Cranial magnetic resonance imaging (MRI) showed improvement in the sellar lesion, and chronic sensorimotor polyneuropathy was diagnosed, ruling out myasthenia gravis. Nivolumab treatment continued. By December 2022, after seven cycles, the patient developed back pain and dysesthesias, with MRI confirming transverse myelitis from C7 to T3. Nivolumab was discontinued, and high-dose corticosteroids (1 g methylprednisolone daily for 5 days) led to clinical improvement. A 12-week taper followed, with no symptom recurrence. Disease progression in April 2023 led to a switch to pazopanib, maintaining a partial response for 6 months.</p><p><strong>Conclusion: </strong>This case emphasizes the serious nature of neurological irAEs from ICIs and the critical need for early detection and management. It also highlights the increased risk of subsequent irAEs after an initial event, underscoring the importance of vigilant monitoring.</p>","PeriodicalId":9625,"journal":{"name":"Case Reports in Oncology","volume":"18 1","pages":"892-899"},"PeriodicalIF":0.7000,"publicationDate":"2025-06-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12240573/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000543929","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Immune checkpoint inhibitors (ICIs) have revolutionized metastatic renal cell carcinoma treatment, significantly improving survival outcomes. However, ICIs are linked to immune-related adverse events (irAEs), which can impact multiple organs. Neurological irAEs, such as myelitis, are rare but potentially severe.
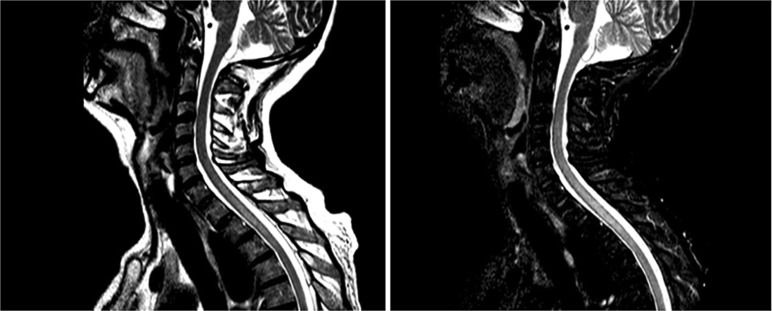
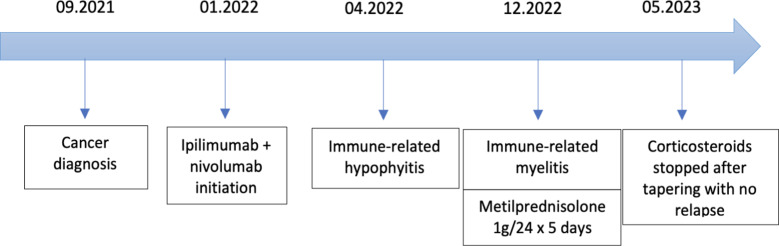
Case presentation: We describe a 54-year-old male with high-grade clear cell renal carcinoma treated with nivolumab and ipilimumab. After four cycles, he developed hypophysitis, adrenal insufficiency, and hypothyroidism, managed with hydrocortisone and levothyroxine, while continuing nivolumab monotherapy. In August 2022, he experienced right eyelid ptosis and right hand weakness. Cranial magnetic resonance imaging (MRI) showed improvement in the sellar lesion, and chronic sensorimotor polyneuropathy was diagnosed, ruling out myasthenia gravis. Nivolumab treatment continued. By December 2022, after seven cycles, the patient developed back pain and dysesthesias, with MRI confirming transverse myelitis from C7 to T3. Nivolumab was discontinued, and high-dose corticosteroids (1 g methylprednisolone daily for 5 days) led to clinical improvement. A 12-week taper followed, with no symptom recurrence. Disease progression in April 2023 led to a switch to pazopanib, maintaining a partial response for 6 months.
Conclusion: This case emphasizes the serious nature of neurological irAEs from ICIs and the critical need for early detection and management. It also highlights the increased risk of subsequent irAEs after an initial event, underscoring the importance of vigilant monitoring.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


