The association between remoteness of injury and in-hospital mortality for motor vehicle collision major trauma patients: evidence of survivor bias in an analysis of registry data.
IF 2.2 3区 医学Q2 PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH
{"title":"The association between remoteness of injury and in-hospital mortality for motor vehicle collision major trauma patients: evidence of survivor bias in an analysis of registry data.","authors":"David J Read, Ian Hayes, Sheena G Sullivan","doi":"10.1186/s40621-025-00586-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Rural Australians have a higher age adjusted rate of both hospitalisation and death from injury, and this rate increases with increasing remoteness. However, it is uncertain if this is due to an increased incidence of injury or less access to treatment. The aim of this study is to examine the association of remoteness and in-hospital mortality in Major Trauma patients admitted to the Royal Melbourne Hospital.</p><p><strong>Methods: </strong>This study was a retrospective cohort study of all persons aged 15 + years diagnosed with 'major trauma', (defined as Injury Severity Score, ISS > 12) from a Motor Vehicle Collision admitted to the Royal Melbourne Hospital from 2010 to 2021. The exposure of interest was remoteness as measured by the Accessibility/Remoteness Index of Australia (ARIA), the outcome of interest was in-hospital mortality. Logistic regression models were constructed looking at the odds of death by increasing remoteness adjusting for age, ISS, and comorbidity. Missing data were imputed using chained equations. A sensitivity analysis was performed for ARIA+ category, and a quantitative bias analysis performed for potential selection bias. All analyses were performed using Stata v17. Ethical approval was obtained from the Melbourne Health Human Research Ethics Committee (HREC2022_044).</p><p><strong>Results: </strong>Eligibility was met for 2324 cases, of whom 53.3% were classified as major city, 36.1% inner regional, and 10.6% outer regional/remote. In-hospital mortality was 6.0% for those injured in major cities, 5.4% in inner regional and 4.1% for outer regional/remote. The median ISS was 19 and 18.3% had at least one limiting comorbidity. The adjusted odds of death were reduced by half for those injured in outer regional and remote compared with major city (OR = 0.51, 95%CI = 0.25-1.03). This result did not alter with the sensitivity analysis for postcode of injury. Quantitative bias analysis suggested the presence of severe selection bias, with the odds ratio showing an increased odds of death (OR = 1.83) for more remotely injured persons.</p><p><strong>Conclusion: </strong>Persons injured remotely are not more likely to die in-hospital after major trauma once they arrive at hospital. Unexpectedly, there was some evidence to suggest that those injured most remotely had a survival advantage, despite similar injury severity Quantitative bias analysis suggested selection bias could be responsible for this apparent survival advantage for more remotely injured persons.</p>","PeriodicalId":37379,"journal":{"name":"Injury Epidemiology","volume":"12 1","pages":"40"},"PeriodicalIF":2.2000,"publicationDate":"2025-07-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12239381/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Injury Epidemiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s40621-025-00586-w","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Rural Australians have a higher age adjusted rate of both hospitalisation and death from injury, and this rate increases with increasing remoteness. However, it is uncertain if this is due to an increased incidence of injury or less access to treatment. The aim of this study is to examine the association of remoteness and in-hospital mortality in Major Trauma patients admitted to the Royal Melbourne Hospital.
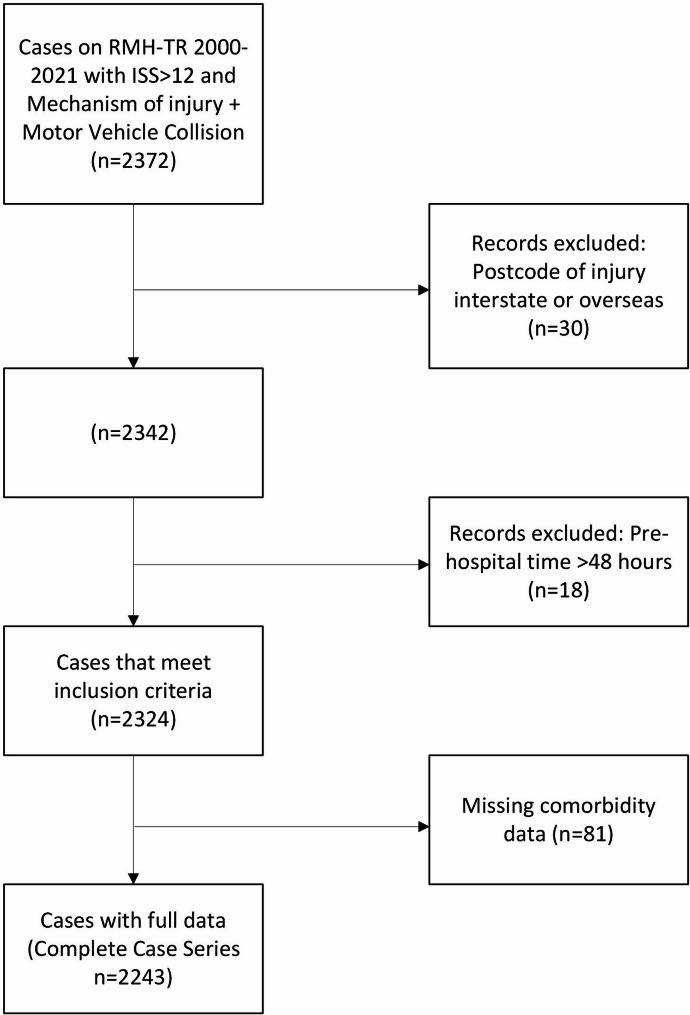
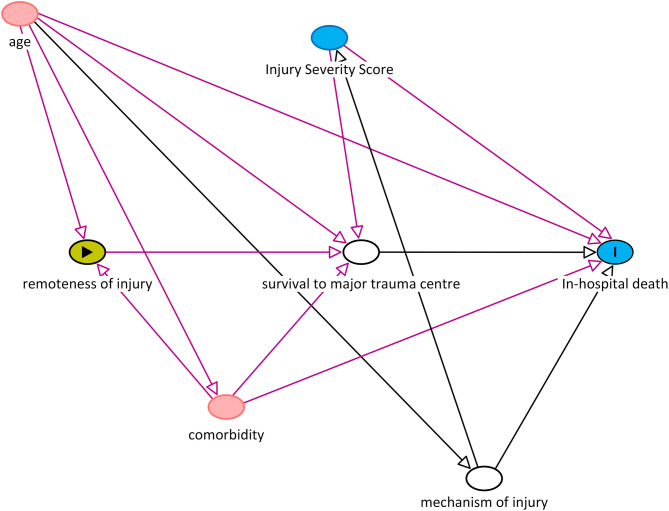
Methods: This study was a retrospective cohort study of all persons aged 15 + years diagnosed with 'major trauma', (defined as Injury Severity Score, ISS > 12) from a Motor Vehicle Collision admitted to the Royal Melbourne Hospital from 2010 to 2021. The exposure of interest was remoteness as measured by the Accessibility/Remoteness Index of Australia (ARIA), the outcome of interest was in-hospital mortality. Logistic regression models were constructed looking at the odds of death by increasing remoteness adjusting for age, ISS, and comorbidity. Missing data were imputed using chained equations. A sensitivity analysis was performed for ARIA+ category, and a quantitative bias analysis performed for potential selection bias. All analyses were performed using Stata v17. Ethical approval was obtained from the Melbourne Health Human Research Ethics Committee (HREC2022_044).
Results: Eligibility was met for 2324 cases, of whom 53.3% were classified as major city, 36.1% inner regional, and 10.6% outer regional/remote. In-hospital mortality was 6.0% for those injured in major cities, 5.4% in inner regional and 4.1% for outer regional/remote. The median ISS was 19 and 18.3% had at least one limiting comorbidity. The adjusted odds of death were reduced by half for those injured in outer regional and remote compared with major city (OR = 0.51, 95%CI = 0.25-1.03). This result did not alter with the sensitivity analysis for postcode of injury. Quantitative bias analysis suggested the presence of severe selection bias, with the odds ratio showing an increased odds of death (OR = 1.83) for more remotely injured persons.
Conclusion: Persons injured remotely are not more likely to die in-hospital after major trauma once they arrive at hospital. Unexpectedly, there was some evidence to suggest that those injured most remotely had a survival advantage, despite similar injury severity Quantitative bias analysis suggested selection bias could be responsible for this apparent survival advantage for more remotely injured persons.
期刊介绍:
Injury Epidemiology is dedicated to advancing the scientific foundation for injury prevention and control through timely publication and dissemination of peer-reviewed research. Injury Epidemiology aims to be the premier venue for communicating epidemiologic studies of unintentional and intentional injuries, including, but not limited to, morbidity and mortality from motor vehicle crashes, drug overdose/poisoning, falls, drowning, fires/burns, iatrogenic injury, suicide, homicide, assaults, and abuse. We welcome investigations designed to understand the magnitude, distribution, determinants, causes, prevention, diagnosis, treatment, prognosis, and outcomes of injuries in specific population groups, geographic regions, and environmental settings (e.g., home, workplace, transport, recreation, sports, and urban/rural). Injury Epidemiology has a special focus on studies generating objective and practical knowledge that can be translated into interventions to reduce injury morbidity and mortality on a population level. Priority consideration will be given to manuscripts that feature contemporary theories and concepts, innovative methods, and novel techniques as applied to injury surveillance, risk assessment, development and implementation of effective interventions, and program and policy evaluation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


